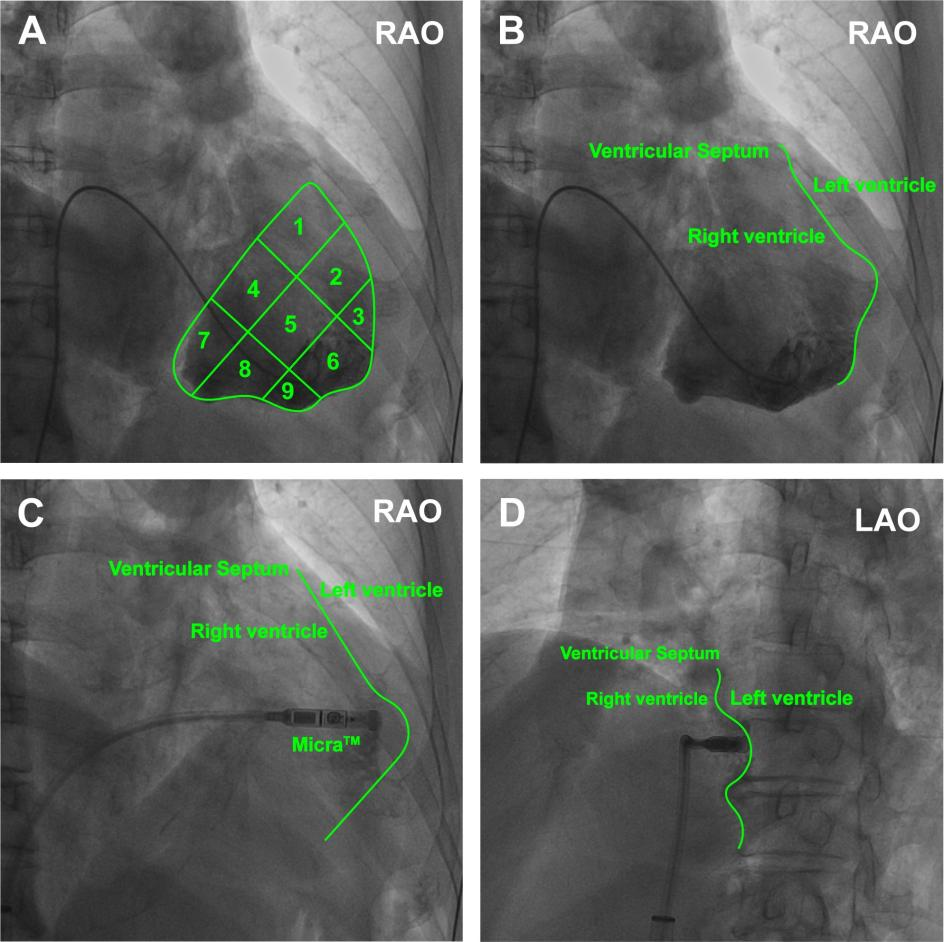
Background: Implanting leadless pacemakers in the right ventricular (RV) apex is prone to causing pericardial tamponade and myocardial perforation. Objective: To investigate the feasibility and safety of right ventriculography-guided implantation of Micra TM leadless pacemaker (Micra) in the RV mid-septum. Methods: 108 consecutive patients who underwent Micra implantation intended in the mid-septum were enrolled and randomized (3:1) into the radiography group (n=81) with assistance of right ventriculography to illustrate the RV septum and the non-radiography group (n=27). All subjects underwent a postoperative computed tomography (CT) scan to determine the Micra location. The Micra location assessed by CT image was compared between the two groups to confirm the accuracy of the intended pacing site. The duration of the procedure, X-ray exposure dose and time were also compared between the two groups. Results: Reconstructed CT 3-D cardiac imaging found the Micra location in the intended mid-septum in 13 patients (48.1%, 13/27) in the non-radiography group and 76 patients (93.8%, 76/81) in the radiography group ( P< 0.0001 between two groups). There was no significant difference in procedure interval between the two groups while the X-ray exposure (564.86±112.44 vs. 825.85±156.12mGy, P < 0.0001), X-ray exposure time (7.79±1.43vs. 12.03±2.86 min, P < 0.0001) and the number of fluoroscopy re-positioning (2.79±1.03, vs. 6.41±1.82, P<0.0001) were significantly less in the radiography group than in the non-radiography group. No implantation-related complications were observed in both groups. Conclusion Right ventriculography increases the accuracy of Micra TM pacemaker implantation in the mid-septum and reduces X-ray exposure.