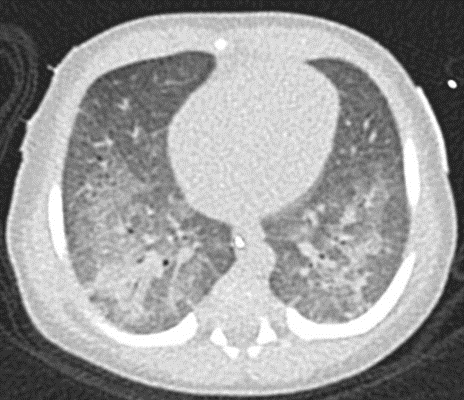
Title page:Title: Beyond the Usual Suspects: Neonatal Fever and DesaturationAuthors: Karolína Doležalová¹, Jana Kodetová¹, Eva Klabusayová², Jana Svobodová ³, Karel Karmazín⁴, Pavel Tkadlec ⁵, Emília Kopecká ⁶, Jan Helešic ⁷Affiliation:₁ Clinic of Paediatrics of the First Faculty of Medicine, Charles University, Thomayer University Hospital, Prague, Czech Republic₂ Department of paediatric anaesthesiology and intensive care medicine, University Hospital Brno and Faculty of medicine, Masaryk University, Brno, Czech Republic₃ Laboratory for mycobacteria, Ifcor- Clinical laboratories, Ltd., Brno, Czech Republic₄ Department of Pediatric Intensive Care, Thomayer University Hospital, Prague, Czech Republic₅ Department of Pulmology, Hospital Uherské Hradiště, Czech Republic₆ Department of Respiratory Medicine, First Faculty of Medicine, Charles University and Thomayer University Hospital, Prague, Czech Republic₇ Department of children’s infectious diseases, The University Hospital BrnoCorresponding author: Karolína Doležalová, MD, PhD, Department of Paediatrics of the First Faculty of Medicine, Charles University, Thomayer University Hospital, Prague, Czech Republic.Orcid: https://orcid.org/0000-0001-7786-8105 karolina.dolezalova@ftn.cz1 IntroductionA one-month-old infant presenting with fever, dyspnoea and desaturation poses a significant diagnostic challenge. The organism in question is notably fragile, exhibiting immature immune functions and the potential for as yet undetected developmental defects. The diagnostic challenge is further intensified in cases where the child is an immigrant, born as a result of an unmonitored pregnancy, born prematurely and with low birth weight. The attending physician must act quickly while carefully untangling the complicated web of different possible diagnoses.2 Case presentationOn the day of admission, the patient was a 31-day-old baby girl born to a Ukrainian mother from an unmonitored pregnancy with a birth weight of 2,350 g. Gestation age unknown. The infant was hospitalised for the first time in the third week of life, having been admitted to the local paediatric ward with a diagnosis of influenza A, which was confirmed by PCR testing of both the infant and her mother. Two weeks later, the infant was readmitted to hospital with a cough, dyspnoea and fever. The laboratory parameters of inflammation were elevated (CRP 188 mg/l, PCT 1,01 ug/l, WBC 26). The presence of bilaterally oriented opacities, suggestive of pneumonia, was evidenced on the chest X-ray. (Figure 1). Empirical antibiotic therapy with piperacillin/tazobactam (Tasocin) has been initiated. From a clinical perspective, the most prominent symptoms were tachypnoea (70 breaths per minute) and signs of increased respiratory effort. The patient experienced apnoeic episodes accompanied by cyanosis and bradycardia, prompting the initiation of high-flow nasal oxygen therapy (HFNO) and transfer to the intensive care unit. Despite ongoing ventilatory support, respiratory insufficiency progressed. Due to persistent tachypnoea, overall deterioration and signs of respiratory acidosis, endotracheal intubation and the initiation of mechanical ventilation were indicated.Figure 1: A: initial chest X ray and initial laboratory markersChallenge pointThe patient is an immature infant who is exhibiting symptoms of dyspnoea, fever and tachypnoea. These symptoms required urgent transfer to a resuscitation care facility and mechanical ventilation. It is evident that the patient exhibits elevated levels of inflammation, as indicated by the presence of significant parameters of inflammation, along with the observation of bilateral opacities on a chest scan. (Podcast 1)Learner reflectionWhat is most likely going on with this patient?What would you do next and why?