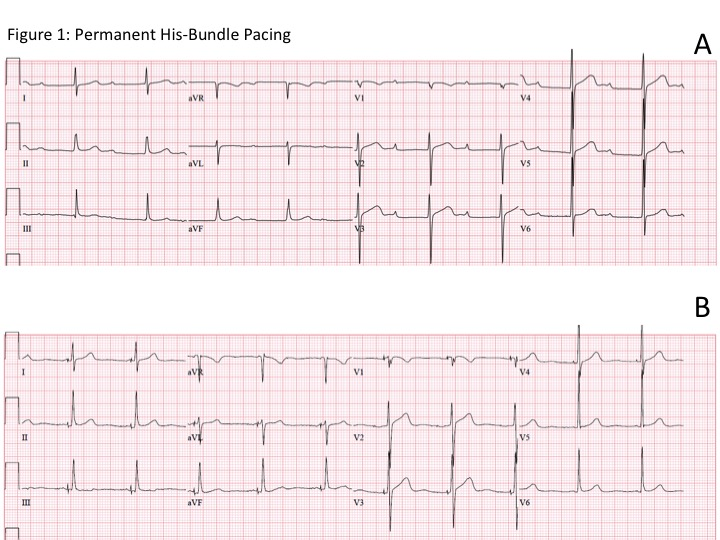
Employing New Criteria for Confirmation of Conduction Pacing – Achieving True Left Bundle Branch Pacing May Be Harder Than Meets the EyeJoshua Sink, MD1, Nishant Verma, MD, MPH2Northwestern University, Feinberg School of Medicine, Department of Internal MedicineNorthwestern University, Feinberg School of Medicine, Division of CardiologyCorresponding Author:Nishant Verma, MD, MPH251 East Huron Street, Feinberg 8-503Chicago, IL 60611312-926-2148Nishant.Verma@nm.orgFunding: NoneDisclosures: Dr. Sink has nothing to disclose. Dr. Verma receives speaker honoraria from Medtronic, Biotronik and Baylis Medical and consulting fees from Boston Scientific, Biosense Webster, AltaThera Pharmaceuticals and Knowledge 2 Practice.Word Count: 1200In recent years, conduction system pacing (CSP) has garnered significant attention from the electrophysiology (EP) community. This movement has been driven by the hypothesis that using the natural conduction system activation is desirable and clinically beneficial in patients with advanced conduction disease and ventricular desynchrony. Permanent His-bundle pacing (PHBP) is generally seen as the purest form of conduction system activation. (Figure 1) PHBP was first described over 20 years ago but the idea has attracted substantial investigative effort in recent years. When successfully achieved, His bundle pacing has been associated with reduction in mortality, reduction in heart failure (HF) admissions, and improvement in left ventricular (LV) function compared to right ventricular (RV) pacing.1 Despite this, consistent achievability in real-world practice remains limited due to a variety of factors including narrow anatomic targetability, lead stability, high pacing thresholds, low ventricular sensing, and inability to correct the QRS in bundle branch block.2Thus, while waiting for the next iteration of improved delivery techniques, pacing leads and programming algorithms,, alternative methods of conductive system pacing have emerged, with the potential to surmount the challenges described.Left bundle branch pacing (LBBP) has recently emerged as an alternative method of CSP. The technique was first described by Huang et al. in 2017 and has seen a momentous rise in interest since.3 In 2019, Huang et al. produced a user manual for a successful LBBP procedure, and in it they attempted to develop the first iteration of criteria for the confirmation of LBBP.4 Utilizing these criteria, or close variations of them, a number of studies were published afterwards that demonstrated preliminary safety, feasibility, and efficacy of LBBP.5,6,7 LBBP became an attractive alternative to His bundle pacing because of the lower thresholds, improved lead stability, and higher procedural success rates. When compared against RV pacing in patients requiring a high burden of pacing, LBBP has demonstrated reduced mortality, HF admissions, and need for upgrade to a BiV device.8 In a small, non-randomized patient sample, LBBP showed greater improvement in LV ejection fraction (EF) compared to BiV pacing.9 Most notably, perhaps, is the astonishing rate of lead placement success, with achievement rates reported as high as 98% in sizable studies.6Differences between the two forms of CSP were apparent from the beginning, including in the appropriate QRS morphology after a successful case. Unlike PHBP, LBBP did not reproduce the native QRS and the QRS duration was often greater than at baseline (Figure 2). The arena of LBBP underwent a notable shift in the Fall of 2021 when Wu et al. proposed new criteria to prove LBBP.10 In this study, they presented an exquisite display of fundamental electrophysiologic principles by using mapping catheters positioned on the His and LV septum during LBB lead placement. Through this painstaking work, they clarified the difference between true LBBP and left bundle branch area pacing (LBBAP), which can incorporate both LBBP and left ventricular septal pacing (LVSP). In their proposed framework, without the presence of a His or LV septum mapping catheter, output dependent QRS transition from non-selective (NS-LBBP) to selective-LBBP (S-LBBP) or LVSP is necessary to prove LBBP and had a sensitivity and specificity of 100%.The present study by Shimeno et al, published in the current issue of the Journal of Cardiovascular Electrophysiology , is the first known effort to document achievement rates of LBBP by utilizing the modified criteria proposed by Wu et al.11 The primary finding of the study is that achieving true LBBP with an acceptable pacing threshold is likely harder than previously realized. As expected, there was improvement after a learning curve, but even in the last third of patients enrolled, the achievement rate of LBBP was only 50%. This is dramatically lower than previously reported achievement rates using the original Huang et al. criteria, and it suggests that not all patients in the previously described studies were actually achieving true LBBP. An unknown subset of patients in these studies was likely only achieving LVSP. This is probably due to a prior reliance on indicators such as a paced right bundle branch block (RBBB) pattern, identification of an intrinsic LBB potential, and/or use of V6 R-wave peak time cutoffs (RWPT) without clear output-dependent QRS transition. It is also worth noting that a variety of RWPT cutoffs have been used seemingly arbitrarily as ‘evidence of LBBP’. This presents a major dilemma and highlights the need for a clear set of LBBP criteria to be defined by the collective EP community. Despite these caveats, many of these previous studies did not fully confirm LBBP in their patients, yet the outcomes from these studies were still clinically promising. This raises the obvious question, does obtaining true LBBP matter? Future studies will need to explore the differences in clinical outcomes between true LBBP and LVSP.Secondarily, Shimeno et al. have provided a useful tool in identifying that LBB potential to QRS-onset ≥ 22ms had a specificity of 98% in predicting LBBP.11 This target measure can help future operators ensure proximal enough engagement of the LBB conduction system. Additionally, the group took a close look at validating a RWPT cutoff time for the prediction of LBBP. Unfortunately, a RWPT cutoff of 68 ms (in non-LBBB patients), determined by the ROC curve, was not highly predictive. This runs contrary to previous reports by Wu et al. and Jastrzebski et al., which reported higher predictive value of RWPT cutoffs10,12 Looking at the data surrounding RWPT cutoffs as a collective, it likely should not be used as a primary metric for confirming LBBP due to imperfect sensitivity and specificity, but it may be an alternative if output dependent QRS transition or change in RWPT of ≥10 ms is not observed. Additionally, in the event that capture thresholds are similar between the LBB and the adjacent myocardium, programmed stimulation is an option to try to reveal a QRS transition by exploiting differences in refractory periods.This study also highlighted one of the unique complications of LBBP by demonstrating a high rate of septal perforation. Paradoxically, more perforations were seen with increased experience, likely highlighting that deeper penetration into the septum is often sought as operators become more familiar with the procedure. The long-term clinical implications of this complication are, thus far, unknown.Looking forward, clear guidelines for confirmation of LBBP need to be defined. This is necessary to ensure quality before undertaking multi-center randomized controlled trials to assess LBBP in comparison to current pacing methods. To date, Wu et al. seem to have provided the best framework to achieve this.10 That said, there are concerns given that this has only been validated in 30 patients (and only 9 with LBBB). In an ideal world, these criteria would be validated in a larger population, though the work to accomplish this would be meticulous given the current gold standard of using an LV septal mapping catheter to prove conduction system capture. Shimeno et al. should be congratulated for their effort in putting this framework to practice. In their work, they have demonstrated that achieving true LBBP as defined by Wu et al. may be harder than meets the eye, and this is very important in assessing the practicality of using LBBP as a widespread alternative to other pacing methods.References:Abdelrahman M, Subzposh FA, Beer D, et al. Clinical Outcomes of His Bundle Pacing Compared to Right Ventricular Pacing. J Am Coll Cardiol . 2018;71(20):2319-2330. doi:10.1016/j.jacc.2018.02.048Zanon F, Abdelrahman M, Marcantoni L, et al. Long term performance and safety of His bundle pacing: A multicenter experience. J Cardiovasc Electrophysiol . 2019;30(9):1594-1601. doi:10.1111/jce.14063Huang W, Su L, Wu S, et al. A Novel Pacing Strategy With Low and Stable Output: Pacing the Left Bundle Branch Immediately Beyond the Conduction Block. Can J Cardiol . 2017;33(12):1736.e1-1736.e3. doi:10.1016/j.cjca.2017.09.013Huang W, Chen X, Su L, Wu S, Xia X, Vijayaraman P. A beginner’s guide to permanent left bundle branch pacing. Heart Rhythm . 2019;16(12):1791-1796. doi:10.1016/j.hrthm.2019.06.016Padala SK, Master VM, Terricabras M, et al. Initial Experience, Safety, and Feasibility of Left Bundle Branch Area Pacing: A Multicenter Prospective Study. JACC Clin Electrophysiol . 2020;6(14):1773-1782. doi:10.1016/j.jacep.2020.07.004Su L, Wang S, Wu S, et al. Long-Term Safety and Feasibility of Left Bundle Branch Pacing in a Large Single-Center Study. Circ Arrhythm Electrophysiol . 2021;14(2):e009261. doi:10.1161/CIRCEP.120.009261Huang W, Wu S, Vijayaraman P, et al. Cardiac Resynchronization Therapy in Patients With Nonischemic Cardiomyopathy Using Left Bundle Branch Pacing. JACC Clin Electrophysiol . 2020;6(7):849-858. doi:10.1016/j.jacep.2020.04.011Sharma PS, Patel NR, Ravi V, et al. Clinical outcomes of left bundle branch area pacing compared to right ventricular pacing: Results from the Geisinger-Rush Conduction System Pacing Registry. Heart Rhythm . 2022;19(1):3-11. doi:10.1016/j.hrthm.2021.08.033Wu S, Su L, Vijayaraman P, et al. Left Bundle Branch Pacing for Cardiac Resynchronization Therapy: Nonrandomized On-Treatment Comparison With His Bundle Pacing and Biventricular Pacing. Can J Cardiol . 2021;37(2):319-328. doi:10.1016/j.cjca.2020.04.037Wu S, Chen X, Wang S, et al. Evaluation of the Criteria to Distinguish Left Bundle Branch Pacing From Left Ventricular Septal Pacing. JACC Clin Electrophysiol . 2021;7(9):1166-1177. doi:10.1016/j.jacep.2021.02.018Shimeno K, Tamura S, Hayashi Y, et al. Achievement Rate and Learning Curve of Left Bundle Branch Capture in Left Bundle Branch Area Pacing Procedure Performed to Demonstrate Output-Dependent QRS Transition.J Cardiovasc Electrophysiol . 2022Jastrzębski M, Kiełbasa G, Curila K, et al. Physiology-based electrocardiographic criteria for left bundle branch capture. Heart Rhythm . 2021;18(6):935-943. doi:10.1016/j.hrthm.2021.02.021Figure LegendsFigure 1: Permanent His Bundle PacingPanel A: A 12-lead electrocardiogram (EKG) shows baseline conduction in a patient with exertional intolerance. The PR interval is markedly prolonged and, with exercise, this patient developed AV block. A permanent His-bundle pacemaker was implantedPanel B: An EKG demonstrating permanent His-bundle pacing in the same patient as panel A. Selective His-bundle capture results in reproduction of the intrinsic QRS complex.Figure 2: Non-Selective Left Bundle Branch PacingA 12-Lead electrocardiogram showing non-selective left bundle branch pacing. The paced QRS morphology is not a direct match for native conduction and the QRS duration is longer than at baseline. However, conduction system capture was confirmed with an output dependent QRS morphology change.FiguresFigure 1: Permanent His-Bundle Pacing