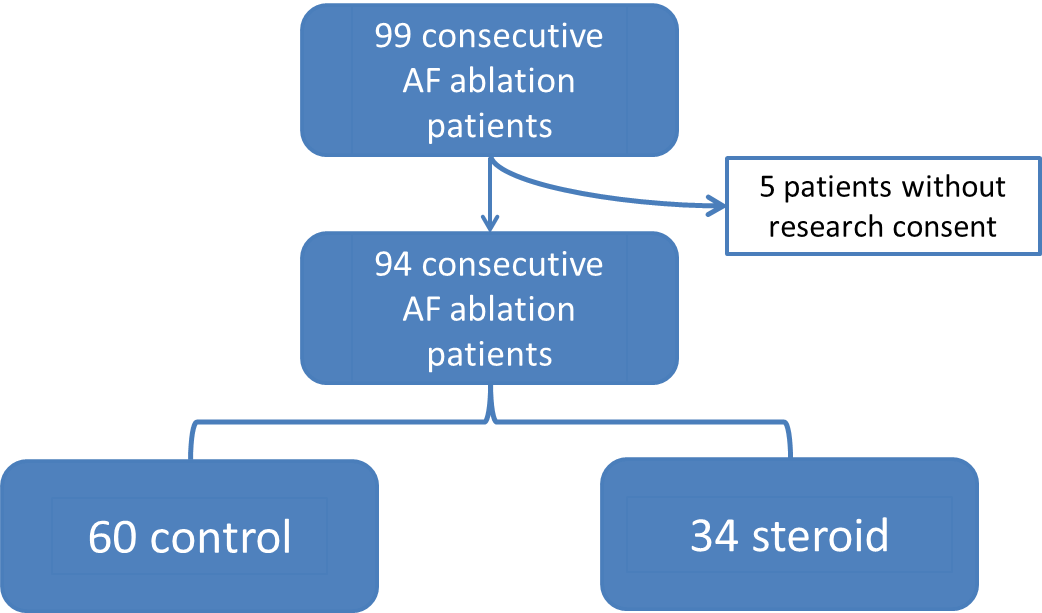
Background: Inflammation is integral in the pathogenesis and propagation of atrial fibrillation (AF). Peri-ablation administration of steroids has been shown to significantly reduce AF recurrence at 3 months. We sought to determine the effect of intraoperative dexamethasone on early recurrence at both 3 months and 12 months post-ablation. Methods: A cohort of 94 adult patients (>18 years) underwent catheter ablation at Mayo Clinic Rochester from January to March 2019. Only first-time ablation patients were included, with all re-do ablations excluded to minimize heterogeneity. Administration of intraoperative dexamethasone 4 mg or 8 mg was determined by chart review from the procedure. At our institution, intraoperative intravenous steroids are administered for postoperative nausea and vomiting (PONV) prophylaxis at the discretion of the anesthesiologist. AF recurrence was determined by ECG or cardiac monitoring at less than 3 months or between 3 months and 1 year with an in-person follow-up visit. Results: A total of 36.2% of patients received intravenous dexamethasone compared to 63.8% who did not (providing a 2:1 comparison group). The incidence of documented AF or flutter lasting greater than 30 seconds was 20.6% in the dexamethasone group versus 21.7% in the non-dexamethasone group, p value 1.00. AF or atrial flutter recurrence from 3 months to 1 year was 20.6% in the dexamethasone group compared to 21.7% in the non-dexamethasone group, p value 1.00. Conclusion: These data suggest that intraoperative intravenous dexamethasone administered during AF ablation for postoperative nausea and vomiting prophylaxis does not have a significant effect on AF recurrence rates.