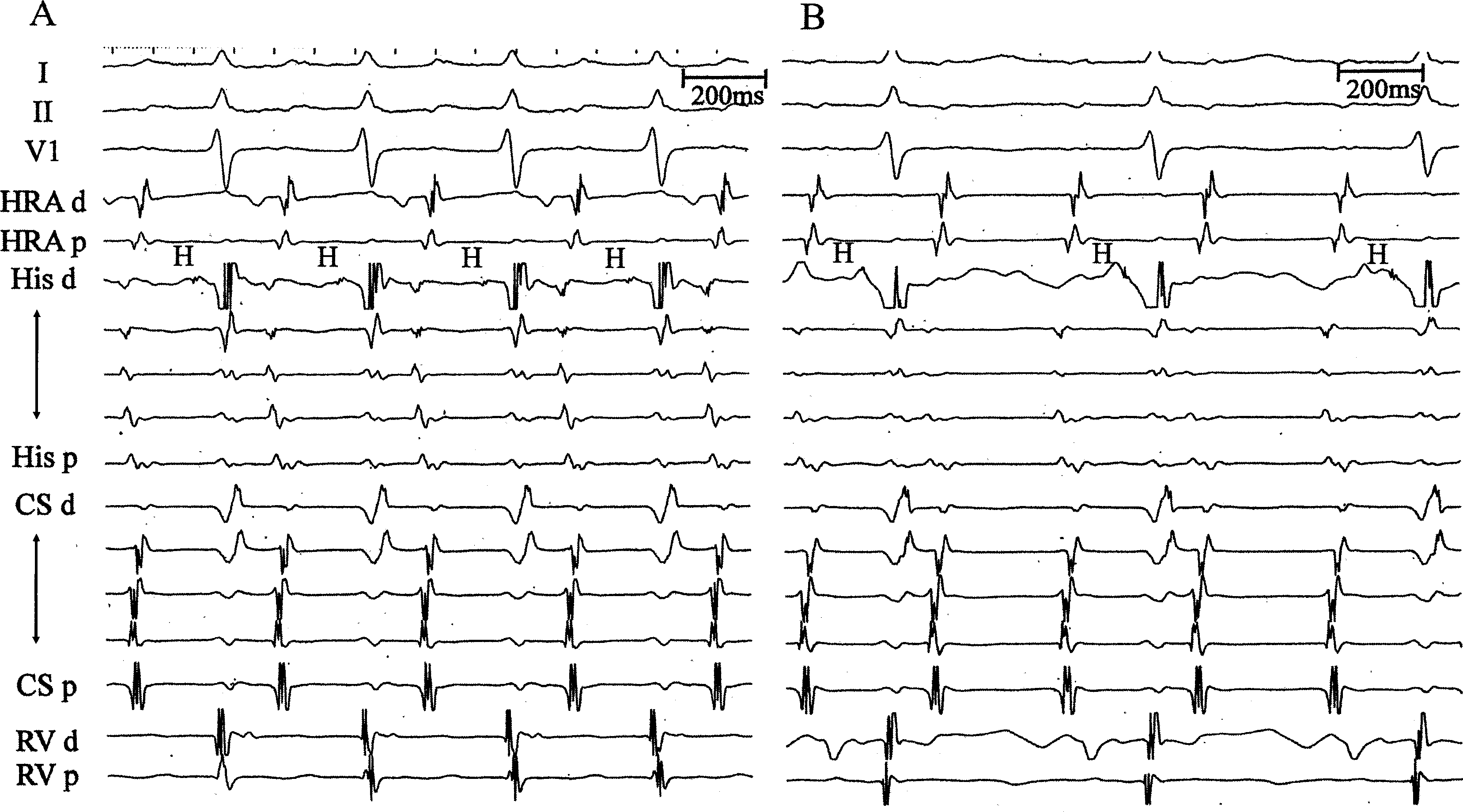
A 77-year-old woman with palpitations was referred for a second radiofrequency ablation for persistent atrial tachycardia (AT). She previously underwent pulmonary vein (PV) isolation for paroxysmal atrial fibrillation, linear ablation between the 3’o clock position of the mitral annulus (MA) and left PV from the endocardium, and ablation inside the coronary sinus (CS) for perimitral atrial tachycardia (PMAT) in the first procedure. A baseline 12-lead electrocardiogram in the second procedure showed stable AT with a cycle length (CL) of 250 ms. No PV reconnection was observed. The CS catheter was placed from 3:30 to 5:00 on the MA, and a proximal-to-distal pattern of CS activation during AT was observed. Activation mapping in the left atrial (LA) endocardium using a three-dimensional mapping system (CARTO3, Biosense Webster, Diamond Bar, CA, USA) revealed a sequence of counterclockwise rotations of the MA. Figures 1A and 1B show the intracardiac electrograms during high-output (20 V) and low-output (5 V) atrial entrainment pacing at a pacing CL of 240ms from CS 3,4, which corresponds to the 4’o clock position of the MA. Dose residual conduction occur across the mitral isthmus (MI) endocardium, epicardium, or both? What is the electrophysiological mechanism during high- and low-output entrainment pacing?