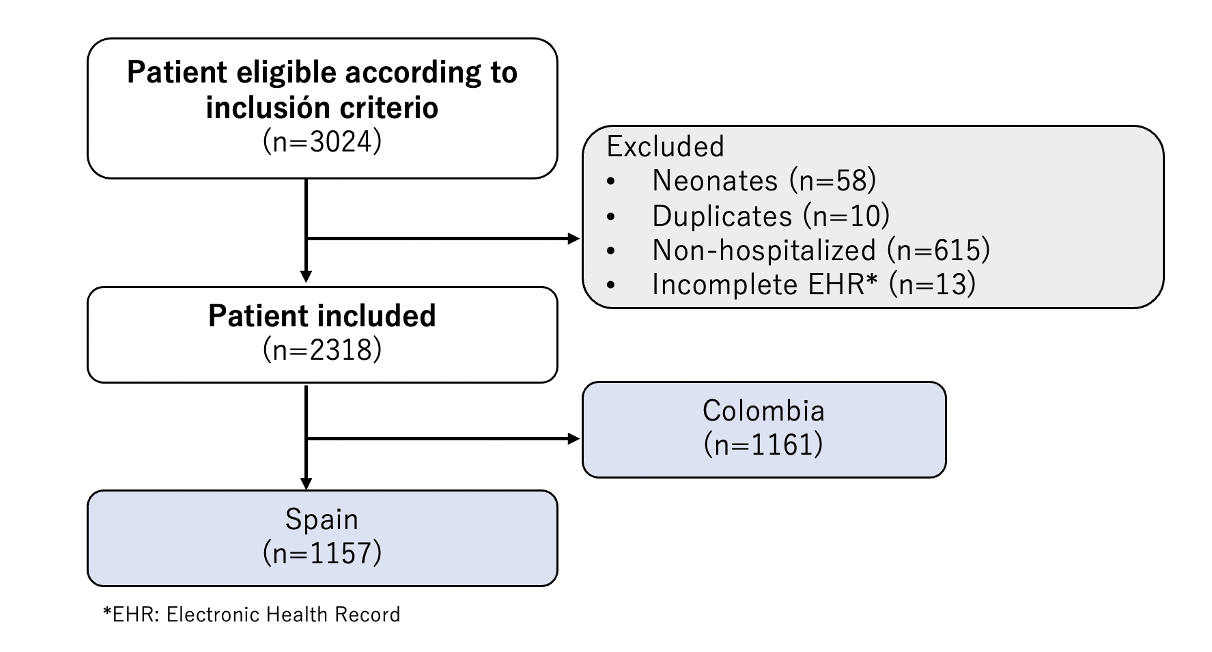
Background: SARS-CoV-2 infection has been extensively documented since the onset of the pandemic, particularly in the adult population. However, there is a lack of evidence describing the phenotypic manifestations of the disease in the pediatric population. We aimed to characterize the clinical phenotypes of SARS-CoV-2 infection in hospitalized children. Methods: The EPICO study is a multicenter cohort conducted between April 2020- November 2021, involving 55 institutions in Spain and 13 institutions in Colombia. Hospitalized children aged 29 days to 17 years with confirmed SARS-CoV-2 infection were included to determine the disease´s evolution, severity factors, and outcomes. Cluster analysis was conducted to characterize clinical phenotypes. Results: A total of 2318 patients from Colombian and Spanish institutions were included. The population was 55% male, with infants being the largest group (36%). Five distinct phenotype clusters emerged, differing significantly in clinical and epidemiological characteristics. Cluster 1 (26.57%) consisted of infants without comorbidities, with low PICU admission and mortality rates. Cluster 2 (18.5%) had respiratory comorbidities, high co-detection, and mortality rates. Cluster 3 (11.51%) showed fever, gastrointestinal symptoms, and high PICU admission. Cluster 4 (32.09%) had mild unspecific symptoms and low mortality. Cluster 5 (11.3%) included adolescents without comorbidities, with low co-detection and hospitalization rates. Comparable findings were observed in both countries. Conclusion: Our study successfully identified distinct patterns of clinical and epidemiological characteristics associated with SARS-CoV-2 infection in hospitalized pediatric patients. These findings may help shape future guidelines and improve risk stratification in children.