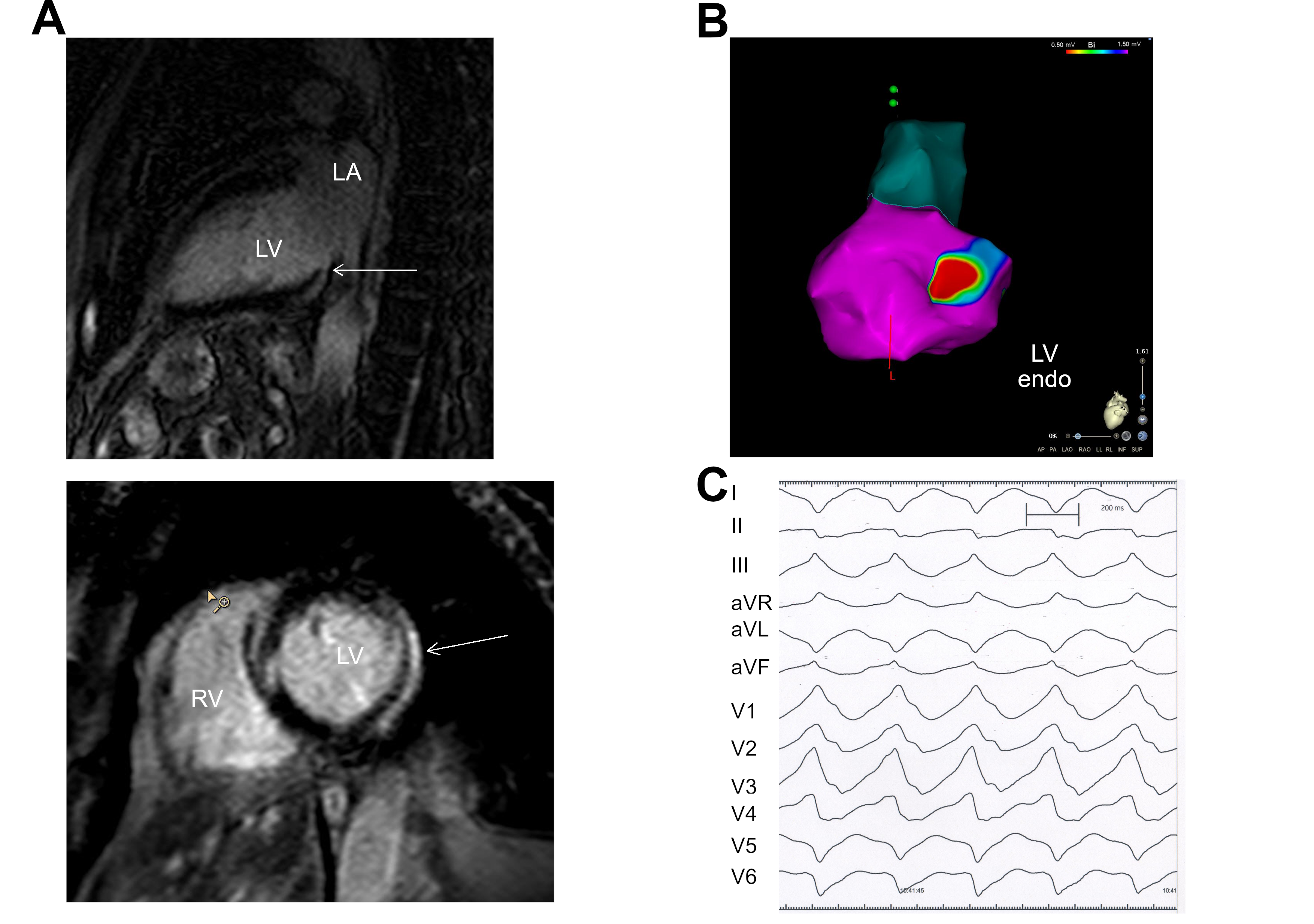
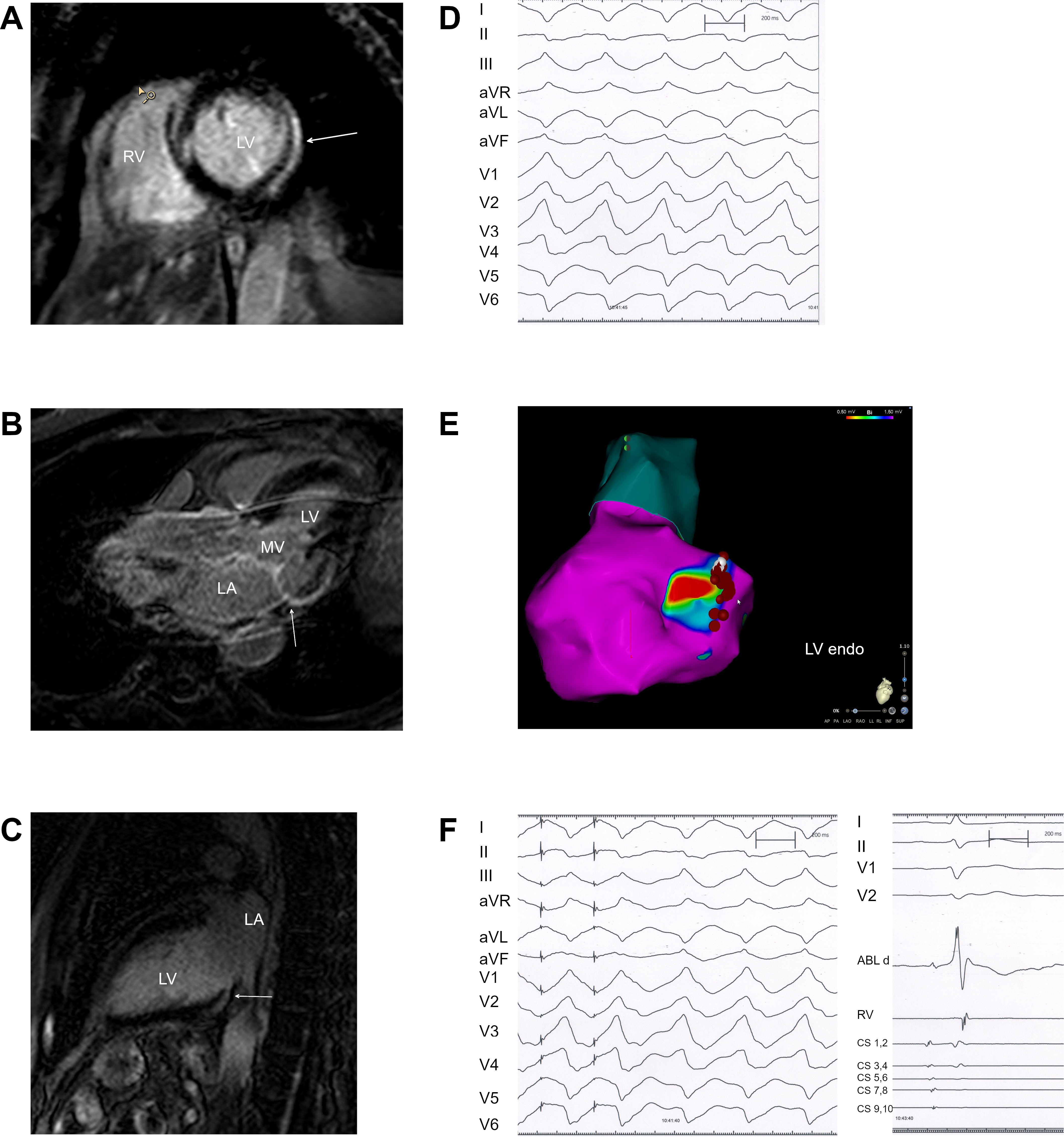
Introduction: Delayed enhancement - magnetic resonance imaging (DE-MRI) has demonstrated that nonischemic cardiomyopathy is mainly characterized by intramural or epicardial fibrosis whereas global endomyocardial fibrosis suggests cardiac involvement in autoimmune rheumatic diseases or amyloidosis. Conduction disorders and sudden cardiac death are important manifestations of autoimmune rheumatic diseases with cardiac involvement but the substrates of ventricular arrhythmias in autoimmune rheumatic diseases have not been fully elucidated. Methods and Results: 20 patients with autoimmune rheumatic diseases presenting with ventricular tachycardia (VT) (n=11) or frequent ventricular extrasystoles (n=9) underwent DE-MRI and / or endocardial electroanatomical mapping of the left ventricle (LV). 10 patients with autoimmune rheumatic diseases underwent VT ablation. Global endomyocardial fibrosis without myocardial thickening and unrelated to coronary territories was detected by DE-MRI or electroanatomical voltage mapping in 9 of 20 patients with autoimmune rheumatic diseases. In the other patients with autoimmune rheumatic diseases, limited regions of predominantly epicardial (n = 4) and intramyocardial (n = 5) fibrosis or only minimal fibrosis (n = 2) were found using DE-MRI. Endocardial low-amplitude diastolic potentials and pre-systolic Purkinje or fascicular potentials, mostly within fibrotic areas, were identified as the targets of successful VT ablation in 7 of 10 patients with autoimmune rheumatic diseases. Conclusion: Global endomyocardial fibrosis can be a tool to diagnose severe cardiac involvement in autoimmune rheumatic diseases and may serve as the substrate of ventricular arrhythmias in a substantial part of patients.