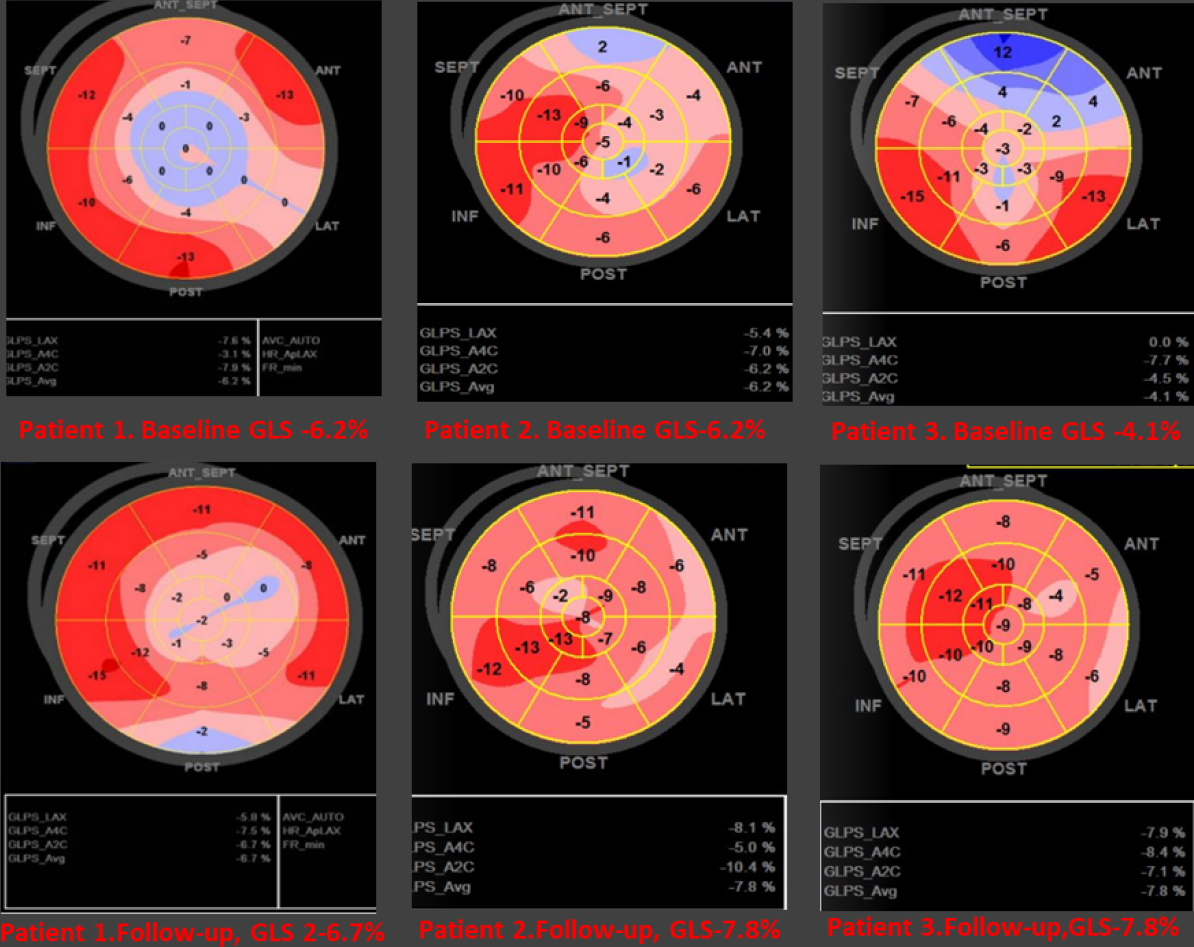
Introduction: Little is known about reverse cardiac remodeling (CRR) under the low-dose S/V therapy. Methods: In 37 patients (mean age 64.5±17.5 years, five females) 24/26mg S/V BID was started. After one month of observation, the following CRR parameters improved: LVEDD (-∆2,9±2.6mm, p<0.01), LVESD (-∆ 2,4±2.5mm, p<0.01), LVEDV(-∆14.6±33.1ml, p=0.04), LVESV (-∆13.4±30.6ml, p=0.04), LAVI (-∆8.7±37.7ml/m2, p<0.01), and EROA (-∆ 0.09 ± 0,01cm2; p=0.03). In opposite to LVEF global longitudinal strain (GLS) changed from -6.6% to -7.9% (absolute improvement of 16%, p <0.001). Walked distance in 6-MWT ( +∆65.4 ± 75.8 m, p <0.001), and the quality of life (MLHFQ 22 vs 16 scores, p<0.01) improved. Decreasing NT-proBNP (-∆ 1,203,1±3,121,4pg/ml, p=0.03) and troponin T (-∆ 4.7±9.4pg/ml, p=0.004) were observed. Correlation between GLS and LVESV (r = -0,43, p = 0.027) was found. ROC curve analysis showed that GLS cut-off value -8% is a good predictor of clinical improvement (6MWT: AUC 0.69 p=0.04) and CRR (MRvol: AUC:0.74 p=0.01; LAVI: AUC 0.71 p=0.04). Conclusion: One-month, low-dose (24/26 mg BID) S/V therapy initiates CRR. GLS’s ability to evaluate LV function is better than LVEF’s. S/V should be started early as patients with symptomatic HFrEF and less impaired LV systolic function (GLS <-8%) are more likely to develop CRR and clinical improvement.