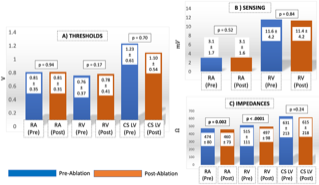
Introduction Catheter ablation (CA) can interfere with cardiac implantable electronic device (CIED) function. The safety of CA in the 1 st year after CIED implantation/lead revision is uncertain. Methods This single center, retrospective cohort included patients who underwent CA between 2012-2017 and had a CIED implant/lead revision within the preceding year. We assessed the frequency of device/lead malfunction in this population. Results We identified 1810 CAs in patients between 2012-2017, with 170 CAs in 163 patients within a year of a CIED implant/lead revision. Mean age 68 ± 12 years (68% men). Time between the CIED procedure and CA was 158 ± 99 days. The CA procedures included AF ablation (n=54, 32%), AV node ablation (n=41, 24%), atrial flutter ablation (n=25, 15%), and PVC/VT ablations (n=24, 14%). The cumulative frequency of lead dislodgement, significant CIED dysfunction, and/or CIED-related infection following CA was (n=1/170, 0.6%). There was a single atrial lead dislodgement (0.6%). There were no instances of power-on-reset or CIED-related infection. Following CA, there was no significant difference in RA or RV lead sensing (p=0.52 and 0.84 respectively) or thresholds (p=0.94 and 0.17 respectively). The RA impedance slightly decreased post-CA from 474 ± 80 Ohms to 460 ± 73 Ohms (p=0.002), as did the RV impedance (from 515 ± 111 Ohms to 497 ± 98 Ohms, p<.0001). Conclusions CA can be performed within 1 year following CIED implantation/lead revision with a low risk of CIED/lead malfunction or lead dislodgement. The ideal time to perform CA after a CIED remains uncertain.