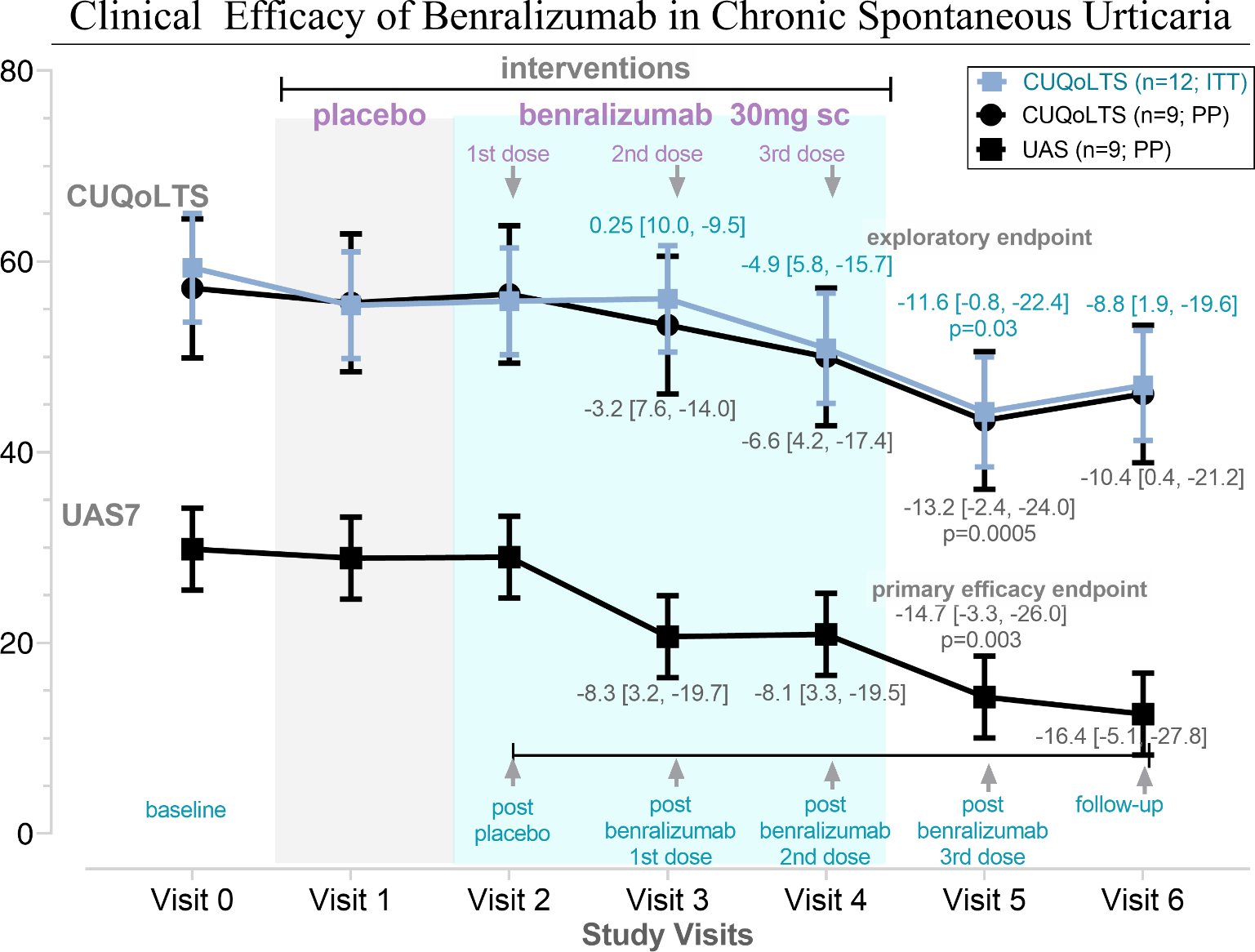
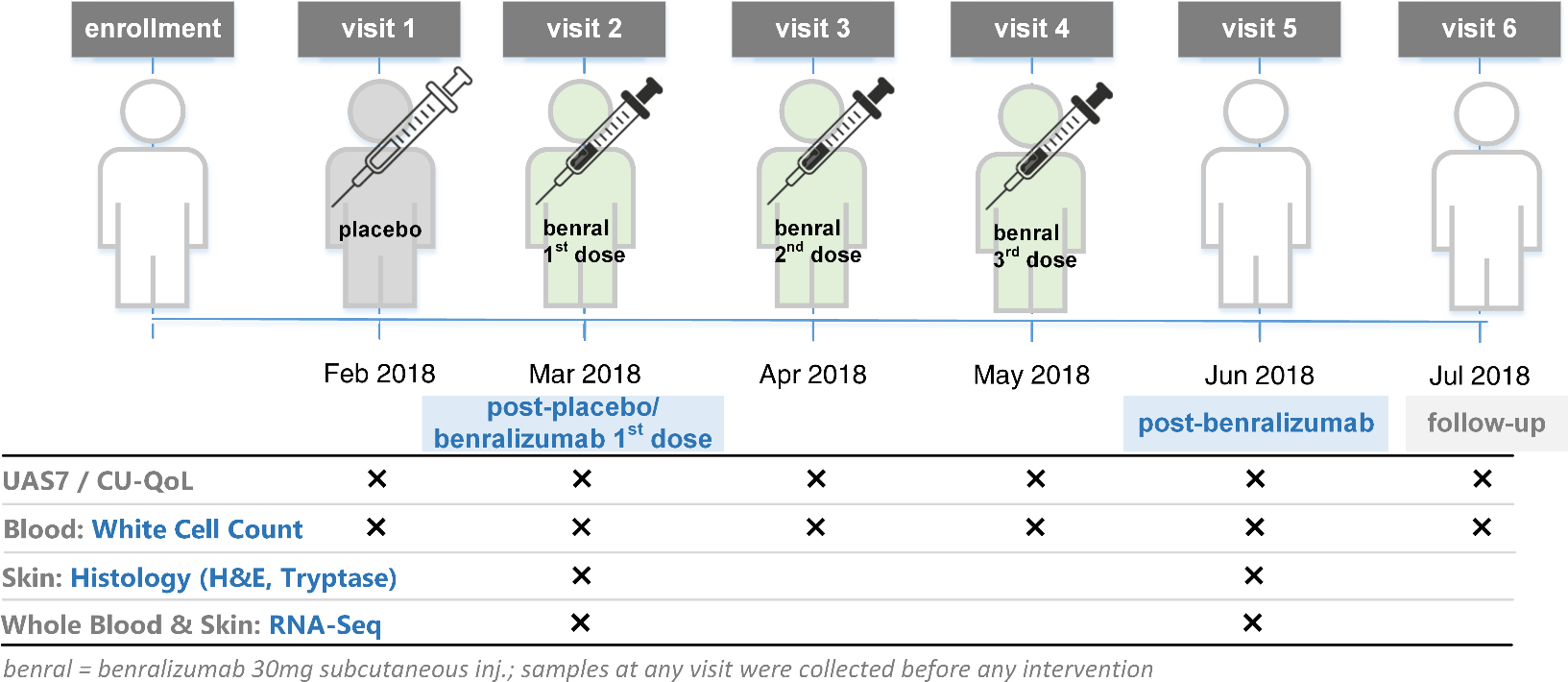
Treatment of Chronic Spontaneous Urticaria With Benralizumab: Report of Primary Endpoint Per Protocol Analysis, and Exploratory EndpointsStandard treatments for chronic spontaneous urticaria (CSU) including the second-generation H1-antihistamines (SGAH) are often ineffective even with four-times the FDA-recommended dose.1,2Eosinophilic infiltrates and an abundance of interleukin-5 (IL5) in CSU lesions (hives) support a role for IL5 in the pathomechanism of CSU.3 Thus, the use of biologic therapies, e.g. benralizumab targeting IL5-receptor-α, in treating SGAH-resistant CSU was hypothesized.A repeated-measures, 24-week study was designed and conducted at an urticaria clinic to determine clinical efficacy of benralizumab in CSU. Twelve SGAH-unresponsive CSU patients (3 males, 9 females; 2 blacks, 10 whites; between ages 32-65 years) having a median daily Urticaria Activity Score (UAS7)4 of 4, and pruritus severity ≥2 were enrolled. After a baseline run-in period, subjects were treated with a subcutaneous placebo dose followed by benralizumab 30mg subcutaneously every month (×3 doses) followed by two off-medication monthly-visits. Subject-reported responses to UAS7 and CU-QoL questionnaires were recorded at the monthly visits. The primary and exploratory endpoints were the change in UAS7 and Chronic Urticaria Quality-of-Life Total Score (CUQoLTS) respectively, from 4 weeks after placebo dose (visit 2) to 4 weeks after last dose of benralizumab (visit 5). Nine subjects completed the study; three withdrew after the first benralizumab dose. An intent-to-treat (ITT) analysis (n=12) of the primary endpoint has been reported previously.5Per-protocol (PP) analysis (n=9) of the primary endpoint, and PP vs. ITT of the exploratory endpoint are reported here. It was presumed that lesions were not self-limiting, and any improvement in outcomes during the study were because of intervention. Non-responders to benralizumab were identified if at any time during the 16 weeks after the first benralizumab dose there was <40% improvement in UAS7 from baseline vs. responders if UAS7 was ≤6.The average duration of urticarial symptoms was 7.0 years. Baseline UAS7 and CUQoLTS ranged between 22-42 and 36-95 respectively. Both outcomes significantly improved at visit 5 vs. visit 2 in 7 of 9 (78%) subjects completing the study. The average difference (95% CL) between visit 2 and visit 5 for UAS7, was -15.5 (-4.1, -26.8, p=0.003) and for CUQoLTS, using ITT analysis, was-13.2 (-2.4, -24.0, p=0.0005) or, using PP analysis, was -11.6 (-0.8, -22.4, p=0.03) (Figure-1 ). Five responders reported no hives/pruritus (UAS7=0) at visit 5 or 6.Between responders and non-responders, the average age (51.6 vs. 53, p=0.9) and symptom duration (5 vs. 9 years, p=0.5) did not differ significantly. However, the adjusted mean UAS7 percentage difference, adjusted for symptom duration, age, and blood eosinophils (eos%), from visit 2 till visit 5 was -84% for responders and +7.5% for non-responders, p=0.0009 (Table-1) . The average baseline UAS7 was not statistically significant (27 vs. 37.5, p=0.5) between groups however, the baseline mean difference for eos% was -6±1 (p=0.001), and for basophil% was -1.2±0.2, p=0.02), which were not observed at visit 5 (eos%: 0±1, p=0.9; basophil%: 0.2±0.2, p=0.8) (Table-1 ). Thus, clinical improvement among responders was independent of baseline disease severity. Non-responsiveness to benralizumab, measured by changes in UAS7, are likely due to other mechanistic factors unrelated to eos% which are eliminated by blocking IL-5R with benralizumab(S-Figure-1) .UAS7 and CU-QoLTS values were significantly correlated (r2=0.9, p<0.0001) (S-Table-3) . CU-QoL components that improved significantly were the pruritus/wheal scores, urticarial interference with physical activities, sleep and spare time (S-Table-4) .This study supports the use of benralizumab for treatment of SGAH-unresponsive CSU. Benralizumab-related improvements in UAS7 and CUQoLTS reported here are similar to the efficacy of omalizumab in CSU reported in a previous study (S-Table-5) .6The sustained significant improvement in urticarial lesions based on subject-reported outcomes by benralizumab warrants further investigation of underlying biologic pathways to better elucidate the role of IL-5 in CSU.