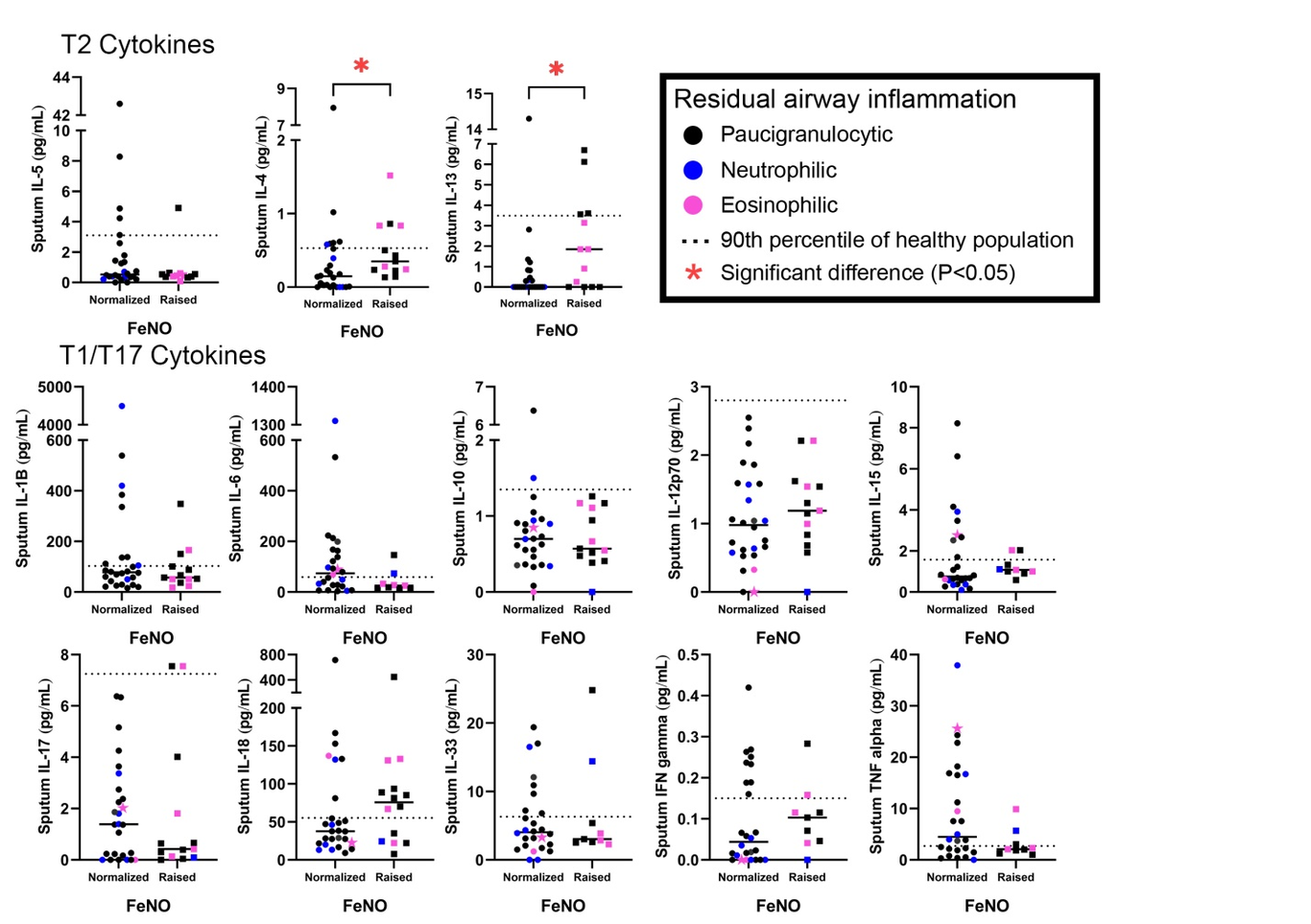
Sputum cytokines associated with raised FeNO after anti-IL5 biologic therapy in severe asthma.To the Editor,Biomarkers such as circulating absolute eosinophil count, % of eosinophils in sputum, and fraction of exhaled nitric oxide (FeNO) are predictors of response to anti-inflammatory therapy for asthma. Failure to normalize FeNO with high doses of corticosteroids are likely to be related to cytokines and chemokines such as IL-5, IL-4, IL-13, eotaxin and TARC derived from eosinophils and other Th2 cells, and alarmins such as TSLP and IL-33 from sources such as the airway epithelium(1). All Anti-IL5 biologics suppress eosinophils in sputum. However benralizumab (anti-IL5RMab) has greater effect in the severe prednisone-dependent patients than mepolizumab/reslizumab (anti-IL5 neutralizing Mab)(2,3). While raised eosinophil count is a predictor of clinical response to anti-IL5 biologics, raised FeNO is often not(4). However, they reduce FeNO to variable levels(4,5) suggesting that FeNO is partly regulated by cytokines derived from eosinophils in the airway(1). The cytokines in sputum associated with raised FeNO in prednisone-dependent severe asthmatics treated with effective anti-eosinophil drugs are not known.In this retrospective observational study, we measured cytokines in sputum using an automated ELISA reader (EllaTM, Protein Simple, R&D Systems, BioTechne, Minneapolis) at baseline and after 4 months of treatment with either benralizumab or mepolizumab/reslizumab and compared the levels of cytokines in those whose FeNO remained high after treatment. Raised FeNO was defined by FeNO >40ppb and an increase of at least 16ppb from pre-treatment value. The study was approved by Hamilton Integrated Research Ethics Board (#11227, 5037), and all patients gave written informed consent. The cytokines assayed were IL-5, IL-4 and IL-13 (Th2 inflammation) and IL-1β, IL-6, IL-10, IL-12p70, IL-15 IL-17A, IL-18, IL-33, IFNγ and TNFα (Th1/Th17 inflammation, Table e3). Details of baseline demographics, methods and statistics are shown in the online supplement.Paired measurements were made in 30 patients who received benralizumab, and 10 each who received mepolizumab/reslizumab. Overall, as previously reported(5), FeNO levels were not significantly reduced by anti-IL5 treatment (median FeNO pre-treatment 29 [5-156] vs FeNO post treatment 37 [6-280]; p=0.25; Figure e1). This change in FeNO did not correlate with a reduction of sputum eosinophils (r=-0.24; p=0.16).Among 15 patients, FeNO remained raised after treatment (Table 1). On average, IL-4 and IL-13 were the only cytokines significantly higher in the sputum of these patients compared to those in whom the FeNO values normalized (Figure 1, Figure e2). Within this group, there were patients with raised IL-4 (31%) and IL-13 (15%) and those with normal IL-4/IL-13. A small proportion of those with normal IL4/13 had raised levels of IL-18 or IL-1β (20%). Residual eosinophilic airway inflammation was significantly more present in patients with raised FeNO (30.8% vs 8.1%; P=0.04; Table e2). Patients with raised FeNO remained to have poor asthma control with an ACQ>1.5, however this did not significantly differ from those with a normalized FeNO (ACQ 1.7±0.9 vs 1.4±1.1; P=0.36; Table 1).This study, despite its limitation of retrospective design and small numbers, provide novel information on the cytokine profile in the airways of severe prednisone-dependent eosinophilic asthma patients whose FeNO remain high after anti-IL5 treatment. This is a common clinically encountered situation. Our observations suggest that IL-4/IL-13 are the cytokines most associated with this phenomenon. This may be due to the airway eosinophilia being uncontrolled or due to a non-eosinophilic source of these cytokines. However, there could be non-IL-4/IL-13 related increase in FeNO that may be due to inflammasome activation and through non-Th2 cytokine pathways that may raise the possibility of airway infections or autoimmune activation(6). This has important clinical implication. These patients may not show adequate response to switching to anti-IL4R Mab if their asthma remains uncontrolled. This needs to be evaluated prospectively.References:Couillard S, Shrimanker R, Chaudhuri R, et al. Fractional Exhaled Nitric Oxide Nonsuppression Identifies Corticosteroid-Resistant Type 2 Signaling in Severe Asthma. Am J Respir Crit Care Med 2021; 204: 731-734.Mukherjee M, Forero DF, Tran S, Boulay ME, et al. Suboptimal treatment response to anti-IL-5 monoclonal antibodies in severe eosinophilic asthmatics with airway autoimmune phenomena. Eur Respir J 2020 Oct 8;56(4):2000117. doi: 10.1183/13993003.00117-2020.Mukherjee M, Bhalla A, Venegas-Garrido C, et al. Benralizumab attenuates blood and airway eosinophilia in severe asthmatics with inadequate response to anti-IL-5 neutralizing antibodies [abstract]. Eur Respir J 2022; 60 (suppl 66): 3994; DOI: 10.1183/13993003.Hearn AP, Kavanagh J, d’Ancona G, et al. The relationship between Feno and effectiveness of mepolizumab and benralizumab in severe eosinophilic asthma. J Allergy Clin Immunol Pract 2021; 9: 2093-2096.e1.Nair P, Kjarsgaard M, Armstrong S, Efthimiadis A, O’Byrne PM, Hargreave FE. Nitric oxide in exhaled breath is poorly correlated to sputum eosinophils in patients with prednisone-dependent asthma. J Allergy Clin Immunol 2010; 126: 404-6.Donnelly LE, Barnes PJ. Expression and regulation of inducible nitric oxide synthase from human primary airway epithelial cells. Am J Respir Cell Mol Biol 2002; 26: 144-51.AuthorsPieter-Paul Hekking 1,2, Kayla Zhang1, Carmen Paz Venegas Garrido 1, Raquel Lopez-Rodriguez 1,3, Melanie Kjarsgaard1, Manali Mukherjee 1, Parameswaran Nair 11. Division of Respirology, Department of Medicine, St. Joseph’s Healthcare Hamilton, McMaster University, Hamilton, Ontario, Canada.2. Department of Respiratory Diseases, STZ Centre of Excellence for Asthma & COPD, Franciscus Gasthuis & Vlietland Hospital, Rotterdam, the Netherlands.3. Department of Allergy, Lucus Augusti Hospital, Lugo, SpainCorrespondenceDr Parameswaran NairFirestone Institute for Respiratory HealthSt Joseph’s Healthcare Hamilton50 Charlton Avenue EastHamilton, Ontario, L8N4A6, CanadaTel: 905-522-1155 x 35044Fax: 905-521-6183E-mail: parames@mcmaster.ca