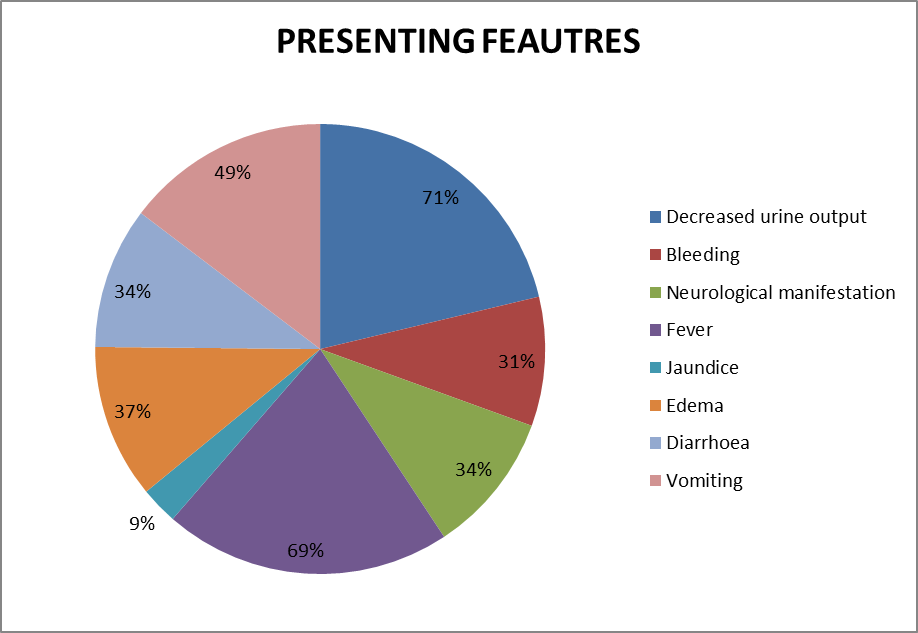
An amiss complement pathway can cause atypical hemolytic uremic syndrome (aHUS) with microangiopathic hemolytic anemia, thrombocytopenia and acute kidney injury. An observational study to understand complement abnormalities and outcome among pediatric aHUS in absence of targeted therapy was done. We enrolled 35 children from July 2017 to December 2018. Besides recording clinical details, hematological and renal parameters were assessed. Complement analysis included a one-time evaluation of C3, C4, anti-factor H antibody (VIDITEST human ELISA kit), factor H, I, B (Sinogeneclon ltd.) and CD46/membrane co-factor protein (MCP) (flow cytometry). SPSS version 23 (Chicago, IL) was used for analysis. Median age was 49 months (sex ratio of 1.7:1). Hypertension was noted in 74.2%(26) and central nervous system involvement in 34.3%(12). At admission, mean hemoglobin was 6.7±1.8 g/dL, median platelet count was 78x109 cells/L(38,101) and median eGFR was 11.91ml/min/1.73m2(6.5, 21.3). C3 was low in 57% (20), while 25.7% (9) had low C4 levels. Anti-factor H antibody was positive in 44% (15). Low expression of MCP in leucocytes was seen in 26.7% (8). Further, 3 had low factor H and high factor B respectively, while 2 had low factor I levels. Plasma-therapy was initiated in 65.7%. Remission was noted in 48.5% (17), 31.4% (11) died and others discontinued treatment. Though anti-factor H antibody is the most common followed closely by low MCP expression, abnormal levels of different complement proteins were observed. Outcome was dismal without eculizumab. We recommend comprehensive complement analysis in pediatric aHUS. Development and availability of targeted therapy remains unquestionable.