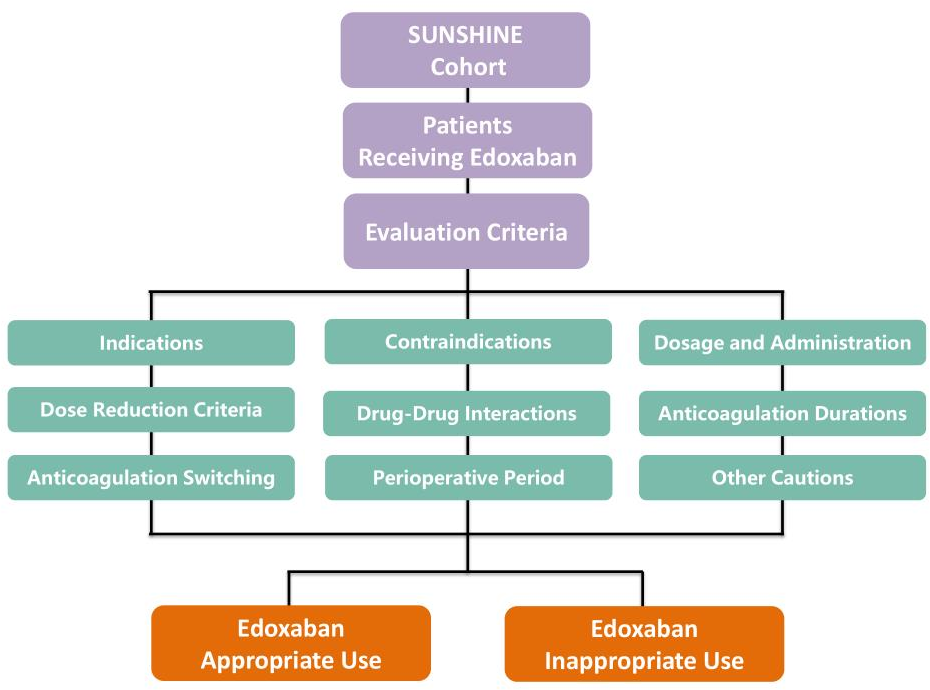
Aim: As the non-vitamin K antagonist oral anticoagulant (NOAC) most recently approved in China, data pertaining to clinical edoxaban use are still scarce. This study investigated the prevalence of and contemporary trends in edoxaban prescription among Chinese patients as well as factors associated with its inappropriate use in a multi-center registry of patients treated in real-world clinical practice. Methods: This real-world, prospective, multicenter, and non-interventional study included 1005 inpatients treated with edoxaban. According to National Medical Products Administration and European Heart Rhythm Association guidelines, edoxaban therapy was determined to be appropriate or inappropriate in each case. Results: The median patient age was 70.0 years (interquartile range, 61.0–78.0 years), and 46.3% were women. Overall, 456 (45.4%) patients received inappropriate edoxaban therapy, and common issues included an inappropriately low (183, 18.2%) or high (73, 7.3%) dosage, wrong drug selection (109, 10.8%), unreasonable off-label use (49, 4.9%), incorrect administration timing (16, 1.6%), and contraindication due to other medications (27, 2.7%). Several factors (e.g., age, weight, kidney function, anemia, and bleeding history) were associated with an increased risk of inappropriate edoxaban therapy, whereas factors associated with cardiovascular specialties (e.g., hospitalized in cardiovascular department and dronedarone or amiodarone use) decreased this risk. Conclusion: In this real-world study, 45.4% of patients received an inappropriate treatment with edoxaban. Multiple clinical characteristics can help identify patients who should receive edoxaban. Further development and implantation of educational activities and management strategies are needed to ensure the correct use of edoxaban.