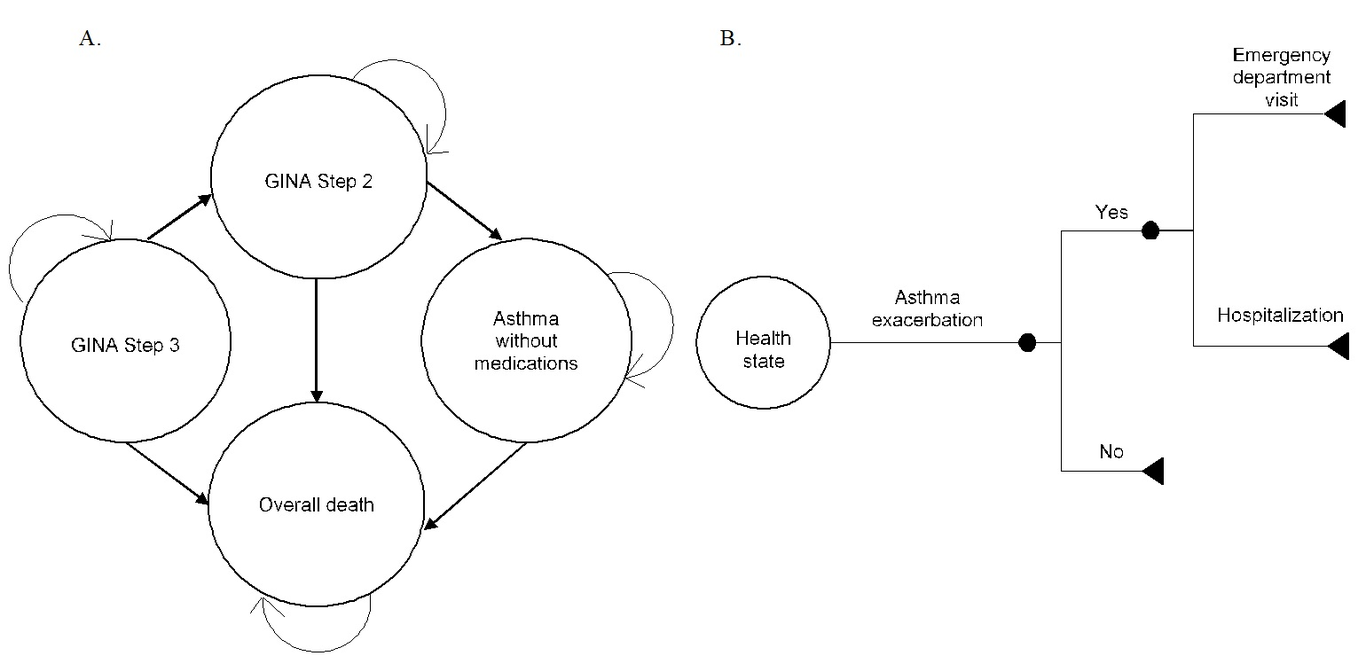
Background: Current cost-effectiveness evaluations of the house dust mite (HDM) allergen immunotherapy fail to account for its effect on the reduction of exacerbations and medications while considering potential differences across patient populations. We aimed to evaluate the cost-effectiveness of subcutaneous immunotherapy (SCIT) plus inhaled corticosteroids (ICS) vs ICS for pediatric and adult patients with allergic asthma (AA) and AA with Allergic rhinitis (AR) from the health care system perspective. Methods: A Markov model with a 3-month cycle length and a 10-year time horizon was developed. A hypothetical cohort of eight years old patients with controlled (or partially controlled) AA was the base case population. Health states were: treatment with GINA Step-3, Step-2, medication-free asthma, and all-cause death. Effectiveness was measured by the reduction in medication doses and exacerbations. Scenario analyses were conducted considering allergic AR as a comorbid condition and an 18-years old cohort at baseline with or without AR. Results: In the base case, the SCIT+ICS would avert 847 exacerbations per 1,000 patients treated and generate additional 0.37 quality-adjusted life years (QALYs) and $836 costs per patient (SCIT+ICS=6.79 QALYs at a cost of $1,438/patient, ICS=6.42 QALYs at a cost of $601/patient). An incremental cost-effectiveness ratio (ICER) of $2,238 per QALY that fall below the willingness to pay threshold was obtained. The SCIT+ICS was also cost-effective among sub-groups of interest: adults win AA (ICER=$2,227) and AA+AR patients (8-years old cohort=$1,628, 18-years old cohort=$1,617). Conclusion: the SCIT+ICS can be cost-effective for pediatric and adult patients with AA with or without AR