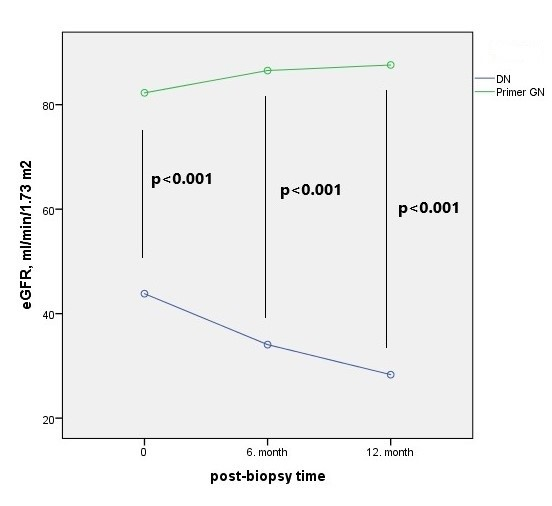
BACKGROUND Primary glomerulonephritis (PGN) has a significant part in non-diabetic kidney disease (NDKD) in diabetes mellitus (DM) patients. In our study, we compared the clinical, demographic, and laboratory features of patients with biopsy-proven diabetic nephropathy (DN) and PGN with type 2 DM METHODS In our retrospective study, type 2 DM patients who underwent kidney biopsy between 2011-2019 were included. Demographic, clinical, and laboratory characteristics of DN and PGN patients were compared. RESULTS Seventy patients with a mean age of 55.7 ± 9.4 and 43 (61.4%) males were included. 38 (54.3%) of the patients had DN, and 32 (45.7%) had PGN. In the PGN, membranous GN (20, 62.5%) was most common. In DN patients, diabetes duration was longer; complications such as retinopathy, neuropathy, hypertension, coronary artery disease, heart failure were more frequent. At the time of renal biopsy, blood sugar, HbA1C, blood pressure, serum albumin, and proteinuria values were similar in 2 groups. The pathological damage findings of kidney biopsy in DN patients were more severe. In the first year after kidney biopsy decrease in eGFR was higher in DN patients, whereas eGFR did not change in PGN patients. CONCLUSION In a diabetic patient, fasting blood sugar, hbA1C, serum albumin, and proteinuria did not differ in the differential diagnosis of DN and PGN, whereas complications of DM (retinopathy, neuropathy, hypertension, coronary artery disease) were more characteristic in differentiation. Detection of PGN in a diabetic patient is crucial for the success of the treatment, according to DN.