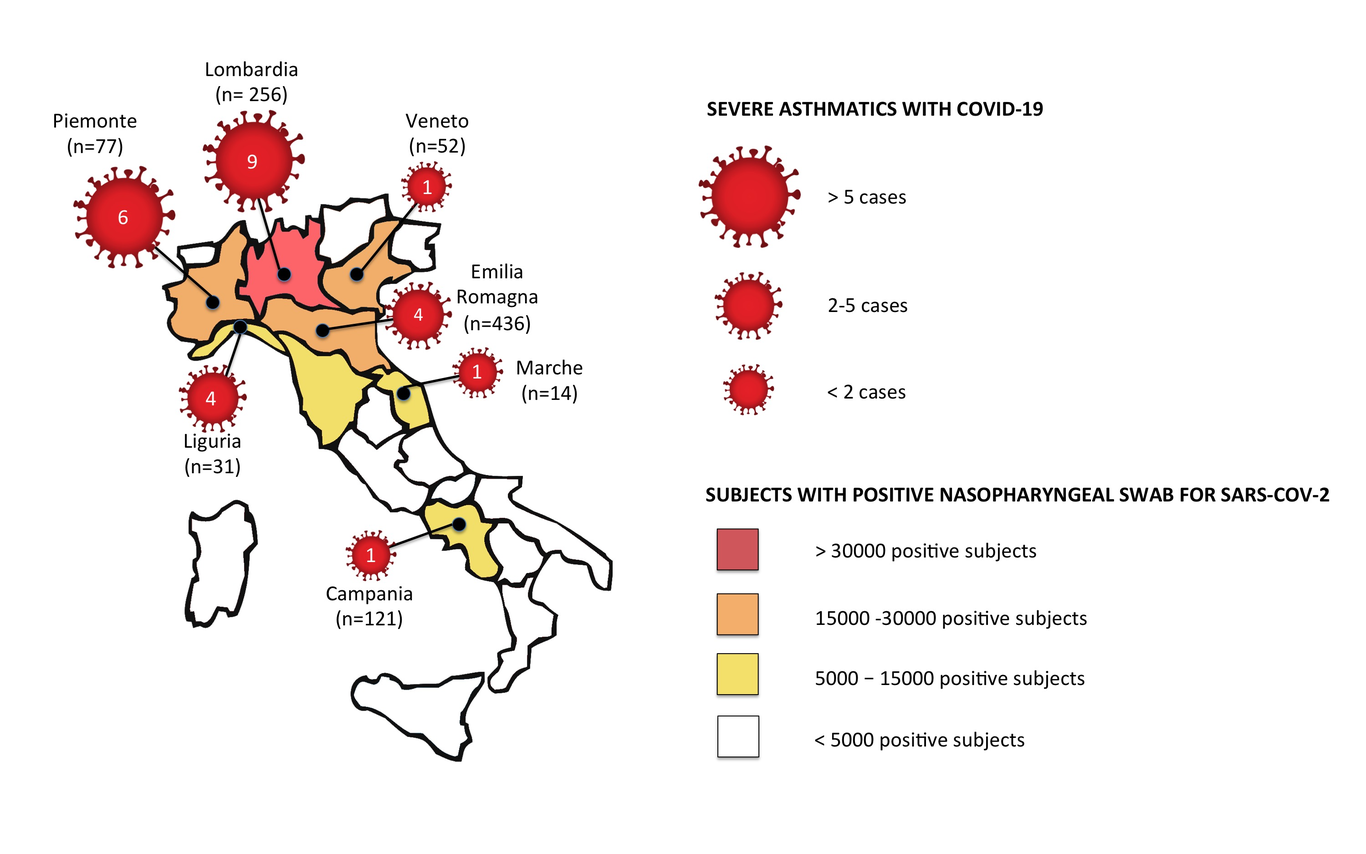
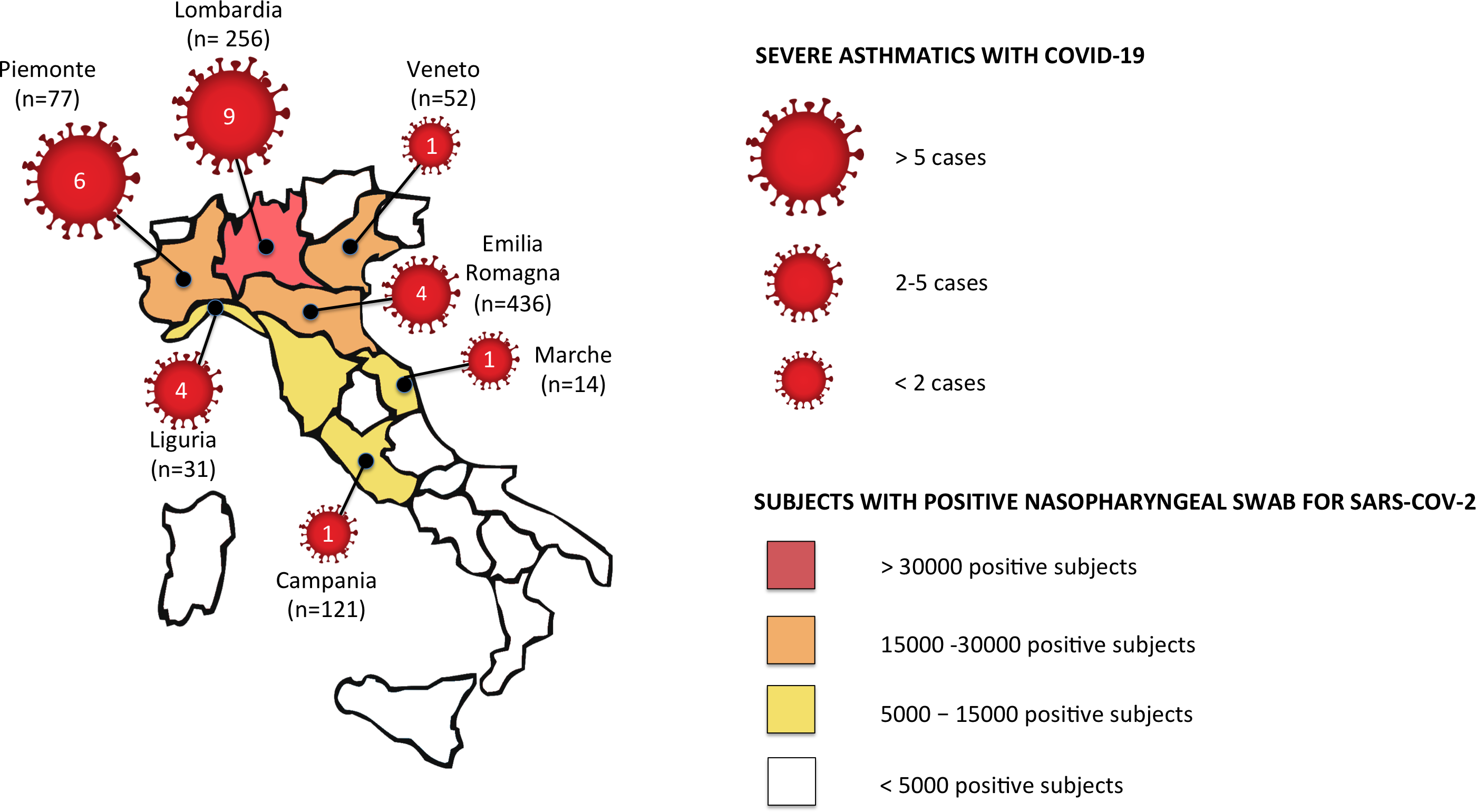
To the Editor Since the end of February 2020 Italy, first non- Asian Country, has reported an ever increasing number of COronaVIrus Disease 19 (COVID-19) patients, which has reached over 200,000 confirmed Severe Acute Respiratory Syndrome-Coronavirus-2 (SARS-CoV-2) infected subjects and resulted in more than 34000 deaths (data updated to June 19th, 20201).Patients with asthma are potentially more severely affected by by SARS-CoV-2 infection 2 and it is well established that respiratory viral infections are associated with severe adverse outcomes in patients with asthma, including increased risk of asthma exacerbation episodes 3. Nonetheless, according to the epidemiological studies published so far, chronic pulmonary diseases are not amongst the most common clinical conditions in COVID-19 patients4About 5-10% of entire asthma population, are severe asthmatics5 and one would expect increased vulnerability to SARS-CoV-2 infection, but no data is so fare available ti confirm this hypothesis.We investigated the incidence of COVID-19, describing its clinical course, in the population of the Severe Asthma Network in Italy (SANI), one of the largest registry for severe asthma worldwide6, and in an additional Center (Azienda Ospedaliero Univeristaria di Ferrara, Ferrara, Italy). All centers, have been contacted and inquired to report confirmed (i.e. patients with positive test result for the virus SARS-CoV-2 from analysis of nasopharyngeal or oropharyngeal swab specimens) or highly suspect cases of COVID-19 (i.e. patients with symptoms, laboratory findings and lung imaging typical of COVID-19 but without access to nasopharyngeal or oropharyngeal swab specimens because of clinical contingencies/emergency) among their cohorts of severe asthma. Demographic and clinical data of the entire cohort of severe asthmatics enrolled in the study and all reported cases of confirmed or suspect cases of COVID-19, have been obtained from the registry platform and collected from the additional Center. Additional data about COVID-19 symptoms, treatment and clinical course have been collected for all cases reported.Ethical issues and statistical analysis are reported in the online supplementary material.Twenty-six (1.73%) out of 1504 severe asthmatics had confirmed (11 out of 26) or highly suspect COVID-19 (15 out 26); eighteen (69.2%) were females and mean age was 56.2 ± 10 years. The geographical distribution of COVID-19 cases is presented in Figure 1.Nine (34.6%) infected patients experienced worsening of asthma during the COVID-19 symptomatic period; four of them needed a short course of oral corticosteroids for controlling asthma exacerbation symptoms.The most frequent COVID-19 symptoms reported were fever (100% of patients), malaise (84.6%), cough (80.8%), dyspnea (80.8%), headache (42.3%) and loss of smell (42.3%). Four patients (15.3%) have been hospitalized, one of which in intensive care unit; among hospitalized patients, two (7.7%) died for COVID-19 interstitial pneumonia. No deaths have been reported among the non-hospitalized patients.Severe asthmatics affected by COVID-19, had a significantly higher prevalence of non-insulin-dependent diabetes mellitus (NIDDM) compared to non-infected severe asthma patients (15.4% vs 3.8%, p=0.002; odds ratio: 4.7). No difference was found in other comorbidities (including rhinitis, chronic rhinosinusitis with or without nasal polyps, bronchiectasis, obesity, gastroesophageal reflux, arterial hypertension, cardiovascular diseases).Twenty-one patients with COVID-19 were on biological treatments: 15 (71%) were on anti-IL-5 or anti-IL5R agents (Mepolizumab n= 13; Benralizumab n=2 - counting for the 2.9% of all severe asthmatics treated with anti-IL5 in our study population) and 6 (29%) were on anti IgE (Omalizumab - 1.3% of all severe asthmatics treated with omalizumab in our study population).Table I summarizes demographic and clinical characteristics of the 26 COVID-19 patients.In conclusion, in our large cohort of severe asthmatics, COVID-19 was infrequent, not supporting the concept of asthma as a particularly susceptible condition to SARS-COV2 infection 2. This is in line with the first published large epidemiological data on COVID-19 patients, in which asthma is under-reported as comorbidity4. The COVID-19 related mortality rate in our cohort of patients was 7.7%, lower than the COVID-19 mortality rate in the general population (14.5% in Italy 1). These findings suggest that severe asthmatics are not at high risk of the SARS-CoV-2 infection and of severe forms of COVID-19. There are potentially different reasons for this. Self-containment is the first, because of the awareness of virus infections acting as a trigger for exacerbations, and therefore they could have acted with greater caution, scrupulously respecting social distancing, lockdown and hygiene rules of prevention, and being more careful in regularly taking asthma medications.Another possible explanation stands in the intrinsic features of type-2 inflammation, that characterizes a great proportion of severe asthmatics. Respiratory allergies and controlled allergen exposures are associated with significant reduction in angiotensin-converting enzyme 2 (ACE2) expression 7, the cellular receptor for SARS-CoV-2. Interestingly, ACE2 and Transmembrane Serine Protease 2 (TMPRSS2) (another protein mediating SARS-CoV-2 cell entry) have been found highly expressed in asthmatics with concomitant NIDDM8, the only comorbidity that was more frequent reported in our COVID-19 severe asthmatics.The third possible explanation refers to the possibility that inhaled corticosteroids (ICS) might prevent or mitigate the development of Coronaviruses infections. By definition, patients with severe asthma are treated with high doses of ICS 5 and this may have had a protective effect for SARS-CoV-2 infection.Noteworthy, among the patients of our case-series of severe asthmatics with COVID-19, the proportion of those treated anti-IL5 biologics was higher (71%) compared to the number of patients treated with anti-IgE (29%). Although the number of cases is too small to draw any conclusion, it is tempting to speculate that different biological treatments can have specific and different impact on antiviral immune response. In addition we may speculate of the consequence of blood eosinophils reduction: eosinopenia has been reported in 52-90% of COVID-19 patients worldwide and it has been suggested as a risk factor for more severe COVID-19 9.In conclusion, in our large cohort of severe asthmatics only a small minority experienced symptoms consistent with COVID-19, and these patients had peculiar clinical features including high prevalence of NIDDM as comorbidity. Further real-life registry-based studies are needed to confirm our findings and to extend the evidence that severe asthmatics are at low risk of developing COVID-19.