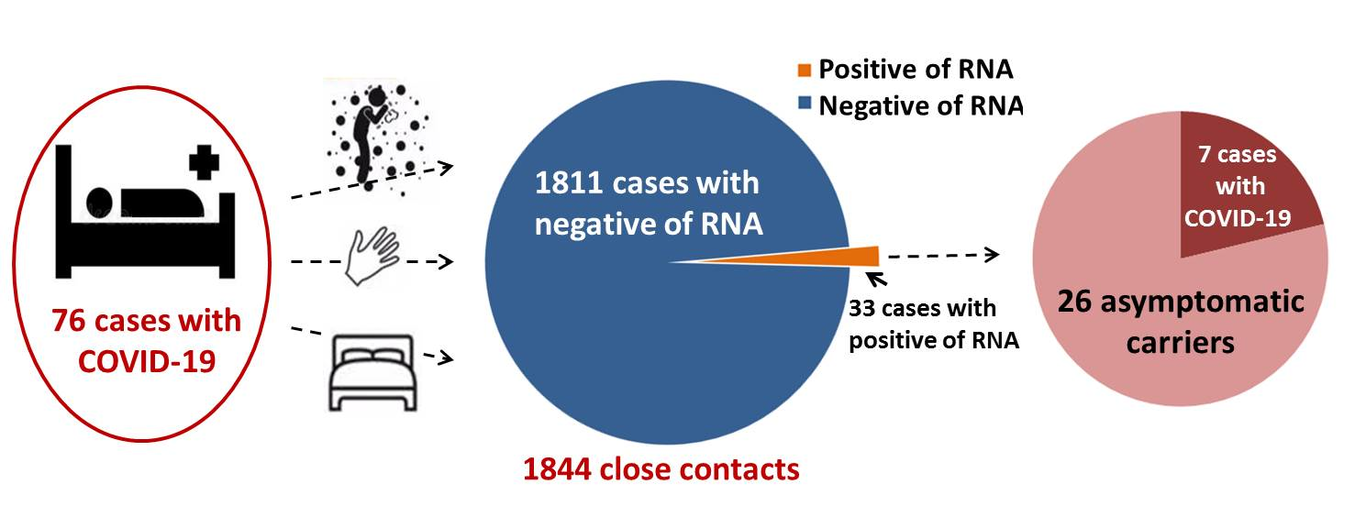
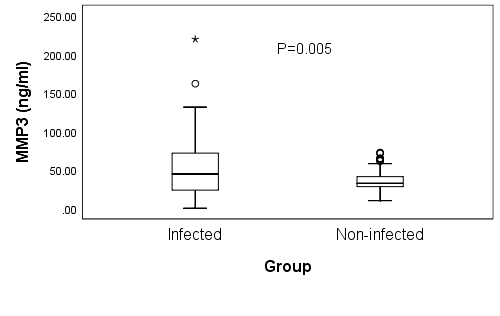
Changes of serum IL-10, IL-1β, IL-6, MCP-1, TNF-α, IP-10 and IL-4 in COVID-19 patientsQingqing Lu1,Zhenhua Zhu2,Chaochao Tan3, Hui Zhou2,Yan Hu2,Ge Shen4,Pan Zhu4,Gang Yang4,Xiaobing Xie2△(1. Hunan University of Chinese Medicine, Changsha Hunan Postal Code: 410208; 2. The First Hospital of Hunan University of Chinese Medicine, Changsha Hunan Postal Code: 410007; 3. Hunan Provincial People’s Hospital, Changsha Hunan Postal Code: 410005; 4.Loudi Center for Disease Control and Prevention,Loudi Hunan Postal Code: 417000)△ Correspondence author, E-mail:xxiaobing888@163.com Abstract: Background and purpose: Studies have shown that some cytokines in COVID-19 patients were elevated. This study aims to assess whether IL-10, IL-1β, IL-6, MCP-1, TNF-α, IP-10 and IL-4 serve as potential diagnostic biomarkers of COVID-19. Methods: The above serum cytokines in COVID-19 patients and non COVID-19 patients were detected by ELISA, SARS-CoV-2 IgM and IgG were detected by chemiluminescence method. Data were analyzed by independent-samples Mann-Whitney U-test, Levene T-test, T’-test or Spearman Correlation test as appropriate. Results: Serum levels of IL-10, IL-1β, MCP-1, TNF-α and IL-4 in COVID-19 patients were significantly higher than those in non-COVID-19 patients, while IL-6 were only significantly higher than in healthy people, IP-10 were significantly lower than in other diseases patients. AUCs of COVID-19 diagnosed by IL-10, IL-1β, IL-6, MCP-1, TNF-α, IP-10 and IL-4 were 0.735, 0.775, 0.595, 0.821, 0.848, 0.387 and 0.682, respectively. In COVID-19 patients’ serum, the levels of IL-10 and MCP-1 of male had noticeably higher than those of female, and all cytokines were significantly positively correlated with age, IL-1β and IL-4 were significantly negatively correlated with IgM, while IL-10, IL-1β, IL-6, TNF-α and IP-10 were significantly negatively correlated with IgG. IL-10 on 43-56 days were significantly lower than at 29-42 days, TNF-α at 15-42 days were significantly higher than at 0-14 days, IP-10 at 0-14 days were the highest, IL-4 at 29-42 days were significant higher than on 0-14 days. Conclusions: The detection of IL-10, IL-1 β, IL-6, MCP-1, TNF-α and IL-4 would assist the clinical study of COVID-19, and targeted inhibition of IP-10 in the early stage may be the key to future treatment of COVID-19.Keywords: cytokine; COVID-19; clinical value; course of disease;Q: What’s already known about this topic?A: Symptoms of COVID-19 patients, infection pathways of SARS-CoV-2, and the COVID-19 patients have higher cytokines.Q: What does this article add?A: What kinds of cytokines in COVID-19 patients were increased, whether they were potential diagnostic biomarkers of COVID-19 and offer prognostic insight upon initial presentation to help guide treatment, their relationship with age, gender,antibody concentration and course of the disease were also discussed.IntroductionNovel coronavirus (SARS-CoV-2) has high infectivity[1,2], the main methods for diagnosing it were nucleic acid detection and serological antibody detection [3]. Inflammatory factors are often increased in severe and critical patients [4], including interleukin (IL), colony-stimulating factor (CSF), chemokine, interferon (IFN), tumor necrosis factor (TNF), chemokine and growth factor (GF) [5]. Most of cytokines are produced by T lymphocytes, fibroblasts and mononuclear macrophages, and can in turn act on these cells, for example, IL-1β can activate vascular endothelial cells and lymphocytes, IL-6 can activate T lymphocytes and induce macrophage activation, MCP-1 can activate mononuclear macrophages, TNF-α can activate fibroblasts, IP-10 can recruit neutrophils and promote the secretion of multiple cytokines, thus, these cytokines could promote each other and jointly mediate inflammation; however, IL-10 can inhibit the inflammatory process. The early symptoms of Coronavirus disease 19 (COVID-19) patients were fever, dry cough and fatigue [6], but severe patients may develop even multiple organ failure [4], which may be related to the levels of cytokines [7-9]. In addition, overactivation of T cells was found in COVID-19 patients [10]. The production of cytokines is related to the individual immune function, so we assumed that the severity of COVID-19 can be predicted according to their levels. Our study aims to reveal the changes of serum levels in IL-10, IL-1β, IL-6, monocyte chemoattractant protein (MCP)-1, TNF-α, interferon-inducible protein (IP)-10 and IL-4 in COVID-19 patients, and assist clinical treatment of COVID-19. Materials and methods2.1 Specimens77 serum samples from male patients and 43 serum samples from female patients were collected from 48 COVID-19 patients in Loudi Center for Disease Control and Prevention, some of who were repeatedly sampled two to four times, and their ages ranged from 8 to 78 years old. The demographic and characteristics of the study participants have been showed in Table 1. Throat swab samples of these patients, including 2 dead patients and 17 asymptomatic infected patients, were detected by real-time PCR (test kits were purchased from Hunan Shengxiang Biotechnology Company), and the positive results of SARs-CoV-2 nucleic acid were confirmed. The COVID-19 is diagnosed according COVID-19 diagnosis and treatment guideline (Seventh Edition)[4]. Brief description is as follows: with epidemiological history and in line with the relevant clinical manifestations, as well as with new coronavirus etiology or serological evidence can be diagnosed. According COVID-19 diagnosis and treatment guideline (Seventh Edition), most of COVID-19 patients only received general treatment, including bed rest, timely effective oxygen therapy and antiviral treatment. Severe and critical patients generally need to be transferred to ICU for treatment including above treatment and timely organ function support treatment. The patients in this study received antiviral drugs such as interferon alpha, ritonavir, ribavirin and some traditional Chinese medicine, such as Qingfei Paidu decoction. In addition, we also collected the serum of non COVID-19 patients from The First Hospital of Hunan University of Chinese medicine. Among these patients, 53 patients suffered from the malignant tumor, hematological disease, rheumatic immune system disease and other diseases that increase the level of inflammatory factors, and 35 healthy people. All patients and their families had informed consent to the inclusion of the study and authorized to use their test results for the study. 2.2 Methods2.2.1 cytokine detectionThe 120 serum contents of IL-10, IL-1β, IL-6, MCP-1, TNF-α, IP-10 and IL-4 were detected by ELISA reader at 450 nm, the test kits and their standard were purchased from Beijing Human Diagnostics Company (double-antibody sandwich ELISA ), TECAN 200-8 were purchased from Shanghai TECAN Trading Company. Sensitivity: the minimal detectable concentrations for they were 0.0225, 0.0355, 0.0600, 0.0655, 0.0386, 0.0102 and 0.0180 pg/mL; specificity: when 50 ng / ml (100 ng / ml for IL-4) was used for specificity test, they did not react with common interfering cytokines and proteins. For statistical analysis: count the results which lower than the minimum detectable concentrations as half of the minimum detectable concentrations. A hole was added as a blank control. The samples whose OD value exceeds the linear range should be diluted before detection. The experiment was conducted in strict accordance with the instructions in the kit. All the reagents had their own standard. Both the repeatability (coefficient of variation between plates and within plates were less than 10%) and specificity were good. The kit has fixed value quality control and negative and positive control to ensure the accuracy of test results.2.2.2 SAS-COV-2 IgM and IgG antibody detectionThe serum samples of all cases were venous blood of 12 hours fasting without hemolysis or hyperlipidemia. The serum was obtained by centrifugation at 4000 RPM for 10 minutes, the contents of IgG and IgM in these serums were detected by magnetic particle chemiluminescence method, the SAS-COV-2 IgM and IgG test kits were purchased from Shenzhen Yahuilong Biotechnology Company, and 10.00AU/mL was taken as the positive judgment value, patients with results of 8-10AU/mL were retested 3-5 days later. Sensitivity and specificity were 98.5% and 100% when the cut-off value was 10.06 AU/mL; the HOOK effect would not appear when the antibody concentration was lower than 8000AU/mL. The experiment was carried out in strict accordance with the instructions in the kits. All the kits were provided with calibration information and quality control materials, and the repeatability (intra assay coefficient of variation was no more than 8%, and the inter assay coefficient of variation was no more than 15%) and specificity was good.2.2.3 Statistical analysisAll datas were processed by IBM SPSS statistic 21 and were drawn by GraphPad Prism 7. According to the characteristics of data distribution, independent-samples Mann-Whitney U-test was utilized to compare the serum levels of IL-10, IL-1 β, IL-6, MCP-1, TNF - α, IP-10 and IL-4 in different groups (COVID-19 patients, other diseases patients and healthy people) and course; Independent-samples Levene T-test or T’-test was utilized to compare COVID-19 patients in different genders; Spearman Correlation test was utilized to analyze the correlation between the levels of cytokines with ages, IgG and IgM. The difference was statistically significant with bilateral P-value < 0.05.3 Results3.1 Detection of IL-10, IL-1β, IL-6, MCP-1, TNF-α, IP-10 and IL-4 in serum samples of COVID-19 patients, other diseases patients and healthy people by ELISAAfter statistical analysis, as Figure 1 and Table 2 shows, it was found that the levels of IL-10, IL-1β, IL-6, MCP-1, TNF-α and IL-4 in the serum of COVID-19 patients were significantly higher than that in the serum of healthy people (PIL-10=0.000, PIL-1β==0.000, PIL-6=0.000, PMCP-1=0.000, PTNF-α=0.000, PIL-4=0.002, respectively), while the serum levels of IP-10 between COVID-19 patients and healthy people were not significant different (P = 0.310); the serum levels of IL-10, IL-1β, MCP-1, TNF-α and IL-4 in COVID-19 patients were significantly higher than those in other diseases patients ( PIL-10=0.000, PIL-1β,=0.000, PMCP-1=0.000, PTNF-α=0.000, PIL-4=0.000, respectively), IP-10 in COVID-19 patients were significantly lower than those in other diseases patients (P=0.004), while the serum levels of IL-6 between COVID-19 patients and other diseases patients were not significant different (P = 0.078). In addition, IL-10, IL-6, MCP-1, and IL-4 in other diseases patients were significantly higher than those in healthy people (PIL-10=0.000, PIL-6,=0.000, PMCP-1=0.023, PIL-4=0.002, respectively), while the serum levels of IL-1β, TNF-α and IP-10 between COVID-19 patients and other diseases patients were not significant different (PIL-1β=0.453, PTNF-α=0.147, PIP-10=0.073, respectively).3.2 Diagnostic efficacy of detection of the IL-10, IL-1β, IL-6, MCP-1, TNF-α, IP-10 and IL-4 on COVID-19 by ELISA The abilities of prediction of IL-10, IL-1β, IL-6, MCP-1, TNF-α, IP-10 and IL-4 on COVID-19 were assessed by ROC curve, as Figure 2 shows, the COVID-19 patients were positive, and the other diseases patients and healthy people were negative, and select the tangent point with the largest Youden’s index as the cut-off value. When choose 2.621, 4.898, 1.730, 19.948, 0.110, 7.083 and 4.015 pg/mL respectively as their cut-off value, AUCs of COVID-19 diagnose by IL-10, IL-1β, IL-6, MCP-1, TNF-α, IP-10 and IL-4 were 0.735, 0.775, 0.595, 0.821, 0.848, 0.387 and 0.682, respectively, which means that IL-10, IL-1β, IL-6, MCP-1, TNF-α and IL-4 have potential diagnostic value for COVID-19, and TNF-α and MCP-1 have the best predictive effect. The sensitivities of diagnosis of TNF-α, MCP-1, IL-1β, IL-10, IL-4 and IL-6 were 81.2%, 84.6%, 63.2 %, 65.8 %, 67.5% and 72.6%, and the specificities of they were 93.0%, 69.8%, 95.3%, 89.5%, 100% and 64.0%; the sensitivity (parallel experiment) and specificity (series experiment) of combined diagnosis of TNF-α and MCP-1 were 97.1% and 97.9%, respectively. 3.3 The relationship between serum levels of IL-10, IL-1β, IL-6, MCP-1, TNF-α, IP-10 and IL-4 with gender and age in COVID-19 patients According to the statistical analysis, as Table 3 shows, it was found that the serum levels of IL-10 and MCP-1 in male COVID-19 patients were markebly higher than those in female patients (PIL-10=0.038, PMCP-1=0.031, respectively), while the differences of serum levels of IL-1β, IL-6, IP-10, TNF-α and IL-4 between male COVID-19 patients and female patients were not markebly significant (PIL-1β=0.611, PIL-6=0.354, PTNF-α=0.152, PIP-10=0.208, PIL-4=0.225, respectively).Ages of the owners of 7 serum samples were not clearly, the relationship between levels of cytokines and age in the other 113 serum samples of COVID-19 patients were show in Figure 3. According to the statistical analysis, the levels of all cytokines in COVID-19 patients were significant positively correlated with their ages (rIL-10=0.403, PIL-10=0.000; rIL-1β=0.200, PIL-1β=0.034; rIL-6=0.320, PIL-6=0.001; rMCP-1=0.431, PMCP-1=0.000; rTNF-α=0.246, PTNF-α=0.009; rIP-10=0.397, PIP-10=0.000; rIL-4=0.283, PIL-4=0.002, respectively).3.4 The relationship between serum levels of IL-10, IL-1β, IL-6, MCP-1, TNF-α, IP-10 and IL-4 and SAS-COV-2 IgM and IgG SARS-Cov-2 IgM and IgG concentrations in COVID-19 patientsThe correlation analysis of levels of IL-10, IL-1β, IL-6, MCP-1, TNF-α, IP-10, IL-4 and antibody concentration in serum samples of COVID-19 patients were shown in Figure 4. It was found that the levels of IL-1β and IL-4 in COVID-19 patients were negatively correlated with the level of IgM (rIL-1β=-0.206, PIL-1β=0.024; rIL-4=-0.208, PIL-4=0.023, respectively), while there were no significant correlation between the levels of IL-10, IL-6, MCP-1, TNF-α and IP-10 and the concentrations of IgM(PIL-10=0.416, PIL-6=0.056, PMCP-1=0.675, PTNF-α=0.301, PIP-10=0.622, respectively); the levels of IL-10, IL-1β, IL-6, TNF-α and IP-10 were negatively correlated with the level of IgG (rIL-10=-0.222, PIL-10=0.015; rIL-1β=-0.212, PIL-1β=0.020; rIL-6=-0.372, PIL-6=0.000; rTNF-α=-0.185, PTNF-α=0.043; rIP-10=-0.273, PIP-10=0.003, respectively), but there were no significant correlation between the levels of MCP-1 and IL-4 and the concentrations of IgG (PMCP-1=0.082, PIL-4=0.067, respectively).3.5 Changes in serum IL-10, IL-1β, IL-6, MCP-1, TNF-α, IP-10 and IL-4 in COVID-19 patients 47 serum are from patients who eventually died, or asymptomatic infected patients, 3 serum are from whose onset time are unknown, the other 70 serum were be divided into five groups according to the acquisition time from onset: a. 0-14 days, b. 15-28 days, c. 29-42 days, d. 43-56 days and e. 57-70 days. As it was shown in Table 4, IL-10 on 43-56 days were significant lower than those on 29-42 days (P=0.049), TNF-α on 15-42 days were significant higher than those on 0-14 days (Pab=0.030, Pac=0.027), IP-10 on 0-14 days were significant higher than those on 43-56 days, IP-10 on 0-14 days were highest and were significant higher than those on43-56 days (P=0.018), and IL-4 on 29-42 days were significant higher than those on 0-14 days (P=0.018).4 DiscussionWe measured the serum levels of these cytokines in COVID-19 patients and non COVID-19 patients by ELISA, the results showed that the serum levels of IL-10, IL-1β, MCP-1, TNF-α and IL-4 in COVID-19 patients were significantly higher than those in non COVID-19 patients, while IL-6 were only significantly higher than in healthy people, IP-10 in COVID-19 patients were significantly lower than those in other diseases patients. IL-10, IL-1β, IL-6, MCP-1, TNF-α and IL-4 have potential study value for COVID-19, and TNF-α and MCP-1 have the best predictive effect. It should be noted that the serum levels of IL-10 and MCP-1 in male COVID-19 patients were significantly higher than those in the female patients. The serum levels of all cytokines in patients were significantly positively correlated with age. IL-1β and IL-4 were significantly negatively correlated with IgM, while IL-10, IL-1β, IL-6, TNF-α and IP-10 were significantly negatively correlated with IgG. The continuous monitoring of the cured COVID-19 patients showed that the levels of TNF-α on 15-42 days were significant higher than those on 0-14 days, and IL-4 on 29-42 days were significant higher than those on 0-14 days, study shows that ICU patients had higher plasma levels of cytokines than non-ICU patients[1], which suggested that levels of cytokines may related to the severity of the disease, so we assume that the reason for this change is that the disease on 0-14 days is light; IL-10 on 43-56 days were significant lower than those on 29-42 days, which may because on 43-56 days, the immune system secreted more IL-10 to induce excessive apoptosis of immune cells in order to avoid damaging its normal tissues in the late stage of inflammation; IP-10 on 0-14 days were highest and were significant higher than those on 43-56 days, the finding that IP-10 rose sharply in the early stages of COVID-19 suggested that targeted inhibition of IP-10 in the early stage might be the key to future treatment of COVID-19. 5 ConclusionTo sum up, we found that the serum levels of IL-1β, MCP-1, IL-6 and IP-10 in patients with COVID-19 were rise, which was same as Severe Acute Respiratory Syndrome (SARS)[11-13], this similarity may be related to the fact that both SARS-CoV-2 and SARS viruses attack Angiotensin-Converting Enzyme 2 (ACE2)[14,15] and produce similar inflammatory processes; TNF-α in patients with COVID-19 were also rise, which was same as Middle East Respiratory Syndrome Coronavirus (MERS)[12,16,17]; what's interesting is that the level of IL-4 and IL-10 also rise in patients with COVID-19, which was different with the another two high pathogenic coronavirus diseases [11-13,16,17]. IL-10, IL-1 β, IL-6, MCP-1, TNF-α and IL-4 would assist the clinical study of COVID-19. In COVID-19 patients, the serum levels of all cytokines were significant positively correlated with age, the poor prognosis of the elderly may be related to this; some of they have relationships with the gender or antibody, the former may be related to the high level of ACE2 in male reproductive system [18-20]; the levels of cytokines would change with the course of disease, and we assumed that targeted inhibition of IP-10 in the early stage may be the key to future treatment of COVID-19. Due to the limited number of samples and enrollment, neither the levels of cytokines between mild and severe patients, were be compared. It has been reported that there are high levels of Pro-inflammatory cytokines in severe COVID-19 patients serum [1,16,21]. To make it clear that whether the cytokine level can predict the course of disease development of COVID-19 patients, the follow-up research will continue.Data Availability Statements: The datas that support the findings of this study are available on request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions.REFERENCES [1] Chaolin Huang,Yeming Wang,Xingwang Li,Lili Ren,Jianping Zhao,Yi Hu,et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China [J]. Lancet, 2020; 395: 497-506.[2] Hongzhou Lu, Charles W. Stratton, Yi‐Wei Tang. Outbreak of pneumonia of unknown etiology in Wuhan, China: The mystery and the miracle [J]. J Med Virol, 2020; 92: 401-402.[3] Yu Chen, Qianyun Liu, Deyin Guo. Emerging coronaviruses:genome structure,replication,and pathogenesis [J]. J Med Virol,2020; 92(4):418-423.[4] The national health and Health Committee and the office of the State, Administration of traditional Chinese medicine (TCM).Diagnosis and Treatment Protocol for COVID-19 (Trial version 7)(state health office Medical Letter No.184 (2020). [EB/OL].(2020-03-04) [2020-03-05] http://www.nhc.gov.cn/yzygj/s7653p/202003/46c9294a7dfe4cef80dc7f5912eb1989.shtml.[5] Chousterman Benjamin G, Swirski Filip K, Weber Georg F. Cytokine storm and sepsis disease pathogenesis. [J]. Seminars in immunopathology,2017; 39(5):517-528.[6] Jasper Fuk-WooChan, Shuofeng Yuan, Kin-Hang Kok, Kelvin Kai-Wang To, Hin Chu, Jin Yang, et al. A familial cluster of pneumonia associated with the 2019 novel corona virus indicating person to person transmission: a study of a family cluster [J]. Lancet, 2020; 395: 514-523.[7] Shimabukuro-Vornhagen Alexander, Gödel Philipp, Subklewe Marion, Stemmler Hans Joachim, Schlößer Hans Anton, Schlaak Max, et al. Cytokine release syndrome. [J].Journal for immunotherapy of cancer,2018; 6(1):56-56.[8] Xue-Qin Meng, Xin-Hua Chen, Zayd Sahebally, Yu-Ning Xu, Sheng-Yong Yin, Li-Ming Wu, et al. Cytokines are early diagnostic biomarkers of graft-versus-host disease in liver recipients [J]. Hepatobiliary & Pancreatic Diseases International,2017; 16(01):45-51.[9] Anne-Britt E Dekker, Pieta Krijnen, Inger B Schipper. Predictive value of cytokines for developing complications after polytrauma [J]. World Journal of Critical Care Medicine,2016; 5(03):187-200.[10] Zhe Xu, Lei Shi, Yijin Wang, Jiyuan Zhang, Lei Huang, Chao Zhang, et al. Pathological findings of COVID-19 associated with acute respiratory distress syndrome [J]. Lancet Respir Med, 2020; 8(4):420-422.[11] Channappanavar Rudragouda, Perlman Stanley. Pathogenic human coronavirus infections: causes and consequences of cytokine storm and immunopathology. [J].Seminars in immunopathology, 2017; 39(5):529-539.[12] Kindler, E., V. Thiel, and F. Weber, Interaction of SARS and MERS Coronaviruses with the Antiviral Interferon Response[J]. Adv Virus Res, 2016. 96: 219-243.[13] Rudragouda Channappanavar, Anthony R. Fehr, Rahul Vijay, Matthias Mack, Jincun Zhao, David K. Meyerholz, et al. Dysregulated Type I Interferon and Inflammatory Monocyte-Macrophage Responses Cause Lethal Pneumonia in SARS-CoV-Infected Mice. Cell Host Microbe, 2016, 19(2): 181-193.[14] Yu Zhao, Zixian Zhao, Yujia Wang, Yueqing Zhou, Yu Ma, Wei Zuo. Single-cell RNA expression profiling of ACE2, the receptor of SARS-CoV-2 [J]. Am J Respir Crit Care Med, 2020, 202(5): 756-759. [15] Yushun Wan, Jian Shang, Rachel Graham, Ralph S. Baric, Fang Li. Receptor Recognition by the Novel Coronavirus from Wuhan: an Analysis Based on Decade-Long Structural Studies of SARS Coronavirus [J]. Journal of virology, 2020; 94(7): e00127-20.[16] Kim Eu Suk, Choe Pyoeng Gyun, Park Wan Beom, Oh Hong Sang, Kim Eun Jung, Nam Eun Young, et al. Clinical Progression and Cytokine Profiles of Middle East Respiratory Syndrome Coronavirus Infection [J].Journal of Korean Medical Science,2016; 31(11):1717-1725. [17] Dianna L. Ng, Farida Al Hosani, M. Kelly Keating, Susan I. Gerber, Tara L. Jones, Maureen G. Metcalfe, et al. Clinicopathologic, immunohistochemical, and ultrastructural findings of a fatal case of Middle East respiratory syndrome coronavirus infection in the United Arab Emirates[J]. Am J Pathol. 2016; 186:652-658.[18] Zhenyu Fan, Liping Chen, Jun Li. Clinical Features of COVID-19-Related Liver Functional Abnormality [J]. Clinical Gastroenterology and Hepatology,2020; 18(7):1561-1566.[19] Caibin Fan, Kai Li, Yanhong Ding, Wei Lu Lu, Jianqing Wang. ACE2 Expression in Kidney and Testis May Cause Kidney and Testis Damage After 2019-nCoV Infection [J/OL]. https://www.medrxiv.org/content/10.1101/2020.02.12.20022418v1, 2020-02-13.[20] Iziah E Sama, Alice Ravera, Bernadet T Santema, Harry van Goor, Jozine M ter Maaten, John G F Cleland, et al. Circulating plasma concentrations of angiotensin-converting enzyme 2 in men and women with heart failure and effects of renin–angiotensin–aldosterone inhibitors[J].Eur Heart J, 2020; 41(19):1810-1817.[21] Lingxi Guo, Dong Wei, Xinxin Zhang, Yurong Wu, Qingyun Li, Min Zhou. Clinical Features Predicting Mortality Risk in Patients With Viral Pneumonia: The MuLBSTA Score. [J]. Frontiers in microbiology,2019; 10:2752.AcknowledgementThe authors promise that all the data are from the clinical, and genuine and believable. The authors report no commercial associations that could be a conflict of interest. Novel Coronavirus Pneumonia Emergency Project of Hunan Province Science and Technology Department (2020SK3009, 2020SK3018, 2020SK3042) and the First-class Discipline Open Fund Project of Hunan University of Chinese Medicine (2018YXJS02) were received in support of this article.