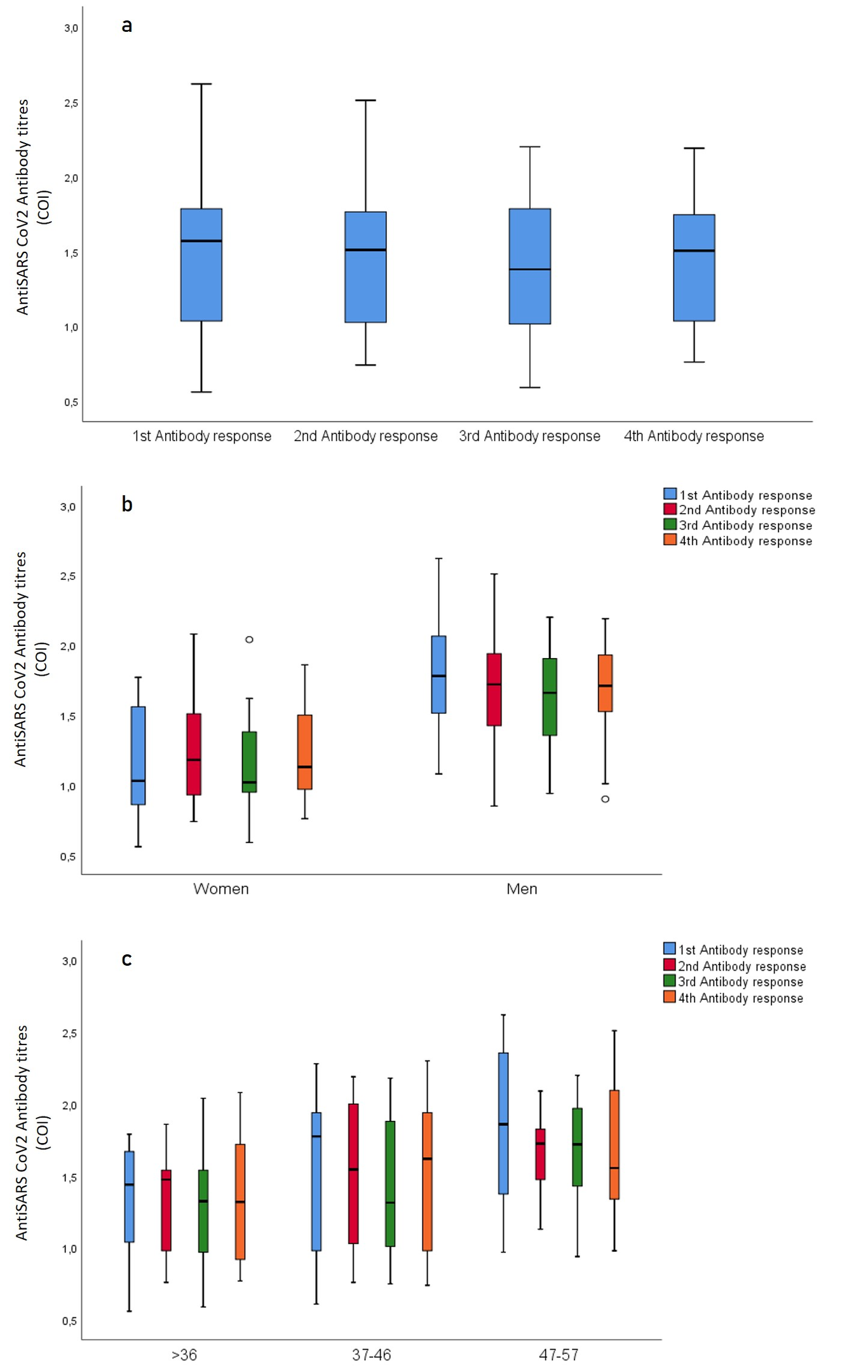
Objective: The severe acute respiratory syndrome-related coronavirus 2 (SARS-CoV-2) and the resulting COVID-19 pandemic pose significant challenges in terms of diagnosis and recurrent infections. Literature data suggest that age, gender and BMI factors are associated with immune response. The first aim of the study was to analyze the change in antibody titer at 15-day intervals until 60 days post symptom onset (PSO) The second aim was to analyze relationship between antibody titer and symptom grade, gender, age, BMI, therapeutic drugs, vitamin supplements, and herbal therapies. Materials and methods: Blood samples were collected from 43 patients (5 mild, 21 moderate, 17 severe diseases), 18 women (41.9 %), and 25 men (58.1 %), on 15, 30, 45, and 60 days PSO after COVID-19 infection. The serum antibody titers were determined by measuring the COVID-19 IgG antibodies by ELISA. Associations between the duration of symptoms, demographic and clinical parameters, medications and vitamins used, and herbal therapies were evaluated by interviewing the participants. Results: Within the first 15 days of illness, 81.4% of the patients were positive. From day 45 PSO, seropositivity was 89.5%. The anti-SARS-CoV-2 antibody titers were statistically higher in men than women at all-time (p<0.01). Antibody titer was higher in older participants compared to younger participants (p<0.02). Plaquenil or Favipiravir use did not effect antibody response (p>0.05). Men had higher fever (p=0.006), shortness of breath (p=0.004), and chest pain (p=0.03) than women. Conclusion: We found powerful antibody response by sixty days PSO, as well as higher antibody response and severity of symptoms in men gender. Data also showed that SARS-CoV-2 antibodies are higher in individuals with older age, whereas BMI, coexisting chronic disease, and drug used had no effect on antibody titers.