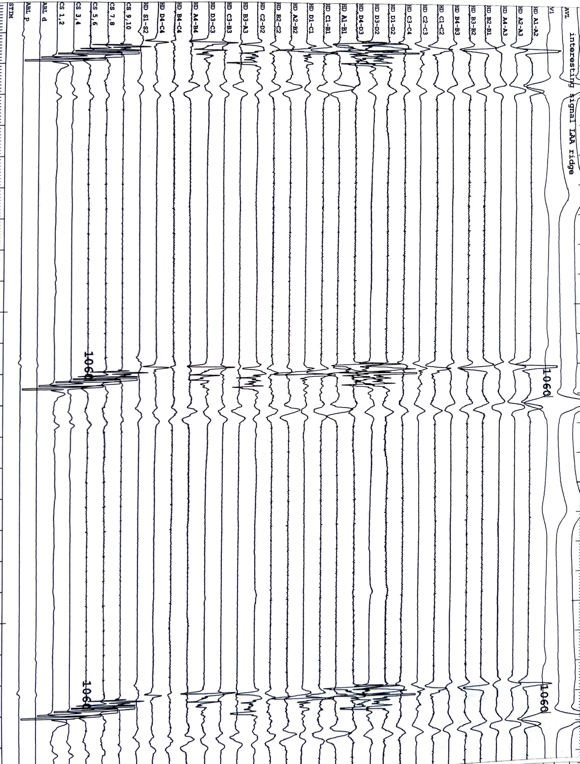
The HD-grid multipolar mapping catheter has emerged as an invaluable tool for greater effectiveness of pulmonary vein isolation (PVI). In the cases described below, fractionated signals seen with the HD-grid catheter at the LAA and LSPV junction were ablated. These signals likely would not be visualized with conventional catheters and may cause recurrences due to incomplete PVI. The directional sensitivity limitations of bipolar electrogram recordings and the unique anatomy of the LAA-LSPV ridge further contribute to the challenge of evaluating pulmonary vein isolation. The HD-grid catheter’s ability to record bipoles parallel and perpendicular to the catheter splines and its high-density mapping capabilities provide a superior means of identifying gaps in ablation and detecting the low-voltage isthmus. Furthermore, factors such as ablation quality, catheter stability, and the thickness of the LAA-LSPV ridge influence the presence of fractionated signals and the success of PVI. Incorporating pre-procedure imaging modalities such as CT or MRI and real-time intracardiac echocardiography could enhance the tailored approach to address these challenges. Future developments in HD-grid technology, including contact force measurement during mapping, may offer additional insights into the nature of these signals. This case series highlights the significance of utilizing the HD-grid catheter for detailed interrogation of the LAA-LSPV ridge, ultimately leading to more effective PVI and improved outcomes in patients with afib