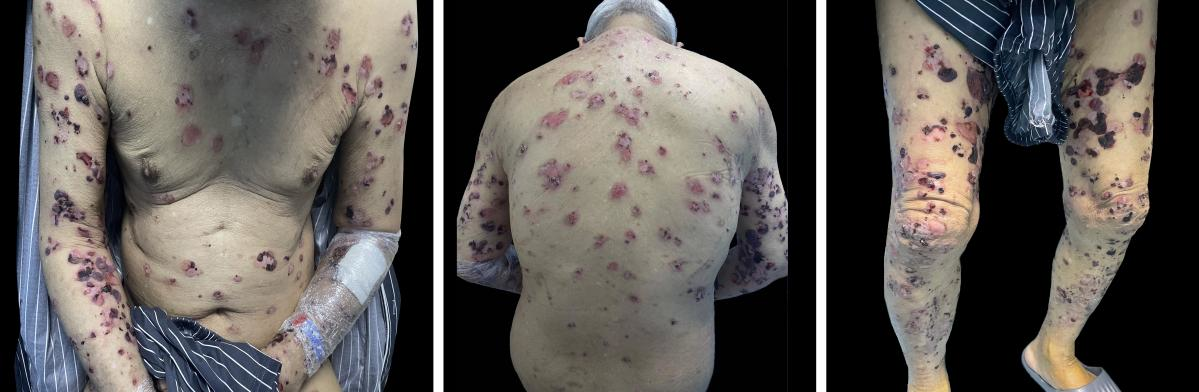
Manuscript category: Letters to the EditorTitle: New-onset bullous pemphigoid after SARS-CoV-2 infectionKeywords: COVID-19, Bullous pemphigoid, SARS-CoV-2Word count: 451 wordsFigure count: 2Table count: 0Sijie Zhou1, Xue Wang1, Lizhi Ma1, Jiaming Fan1, Xinyun Tang1, Peimei Zhou1*1 Department of Dermatovenereology, Chengdu Second People’s Hospital, Qingyun Street, Chengdu, 610041, China.Correspondence to: Peimei Zhou, M.D., Ph.D.Department of Dermatovenereology, Chengdu Second People’s Hospital, Qingyun Street, Chengdu, 610041, China.Tel: +86 18908176315; E-mail: 46551704@qq.comFunding sources: NoneConflict of interest disclosures: All authors declare no conflicts of interest.Data availability statement: Data sharing does not apply to this article as no new data were created or analysed in this study.Ethics statement: The patient consented to publish this information. A 78-year-old male patient with a history of diabetes, hypertension, and renal insufficiency was diagnosed with bullous pemphigoid (BP) after contracting coronavirus disease 2019 (COVID-19). The patient had a positive nasopharyngeal swab for severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) in late December 2022 and was hospitalised for two to three weeks. After discharge, the patient developed erythema and blisters on both hands with itching that gradually involved the whole body. The patient presented to our dermatology department on 3 March 2023.At presentation to the dermatology department, the patient had tense blisters covering the entire body, some of which were breaking down, leaving a small patchy vesicular surface with a yellowish exudate (Fig. 1). Routine blood, procalcitonin, and C-reactive protein tests suggested infection, and a chest computed tomography exam indicated viral pneumonia, consistent with SARS-CoV-2 infection. In addition, the patient’s BP180 antibody levels were >150 U/mL (range: positive >20 U/mL), and rickle cell desmosome antibodies were negative. Furthermore, direct immunofluorescence showed linear basal deposition of immunoglobin G and C3 (uncertain). Finally, histological analyses of an incisional cutaneous biopsy obtained from the patient’s left lower extremity showed the formation of subepidermal blisters containing a few eosinophils, lymphocytes and fibrin, and some epidermal basal cells next to the blisters were edematous, liquefied and deformed.(Fig. 2). These findings were consistent with a BP diagnosis. The patient’s condition did not resolve after conventional treatment with glycyrrhizin, a Chinese herbal extract compound, and other anti-inflammatory treatments; therefore, dupilumab (600 mg initially, then 300 mg every two weeks after) was subcutaneously administered. The symptoms were relieved after two weeks.An increasing number of studies are reporting cutaneous manifestations after COVID-19. For instance, nonspecific skin symptoms, including urticarial lesions, chilblain-like lesions, vesicular eruptions, maculopapular rashes, and livedo, have been reported1,2. We identified no other reports of COVID-19-induced BP but did find a description of BP after SARS-CoV-2 vaccination3. The vaccine mimics antigens to induce specific immune responses in the body, similar to those produced by humans infected with novel coronaviruses, which can cause autoimmune symptoms4. Therefore, our case was likely associated with a novel coronavirus infection.BP is an autoimmune, subepidermal blistering disease occurring in elderly individuals. The exact pathogenesis of BP is unknown, but several factors, such as drugs, thermal or electrical burns, surgical procedures, trauma, ultraviolet irradiation, radiotherapy, chemical preparations, transplants, and infections, may induce or exacerbate BP5. Yet, viral infection-induced BP has rarely been considered. This may be because viruses, as pathogens, can induce cross-reactive autoantibodies sharing epitopes with host cells. Additionally, the virus can directly infect keratinocytes, induce the expression of hidden epitopes, modify existing epitopes, or insert envelope fragments into cells to produce new antigens, which could be responsible for BP development6,7.