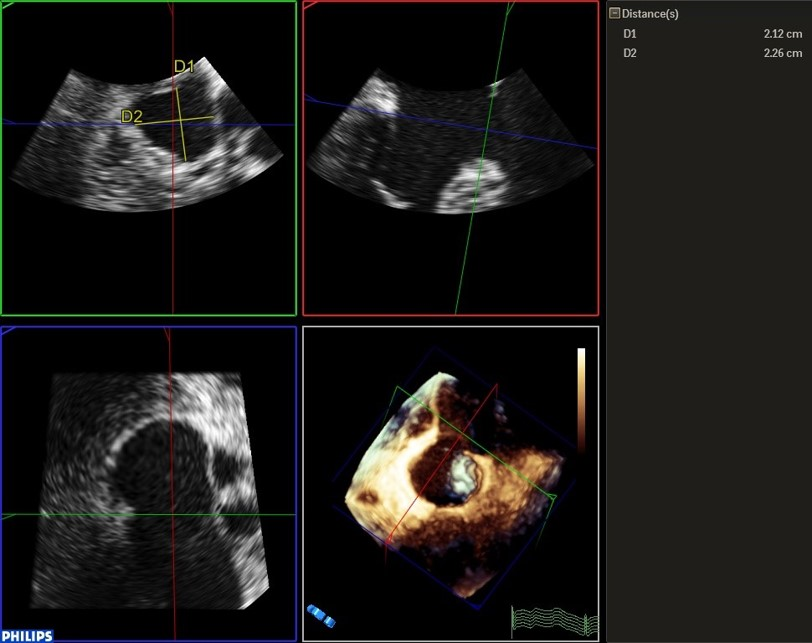
A 60-year-old female was referred to our clinic for evaluation of her rapidly progressive dyspnea, she had no previuos history of heart disease. A murmur was noted on her examination and transthoracic echocardiography was so difficult to be performed due to poor acoustic windows so she was referred to do a transesophageal echocardiography that showed an ostium primum atrial septal defect (ASD) with left to right shunt and a quadrileaflet mitral valve with severe regurgitation. Later on, she underwent surgery with Ostium Primum ASD closure by a patch and double cleft repair by suture after right heart catheterization.