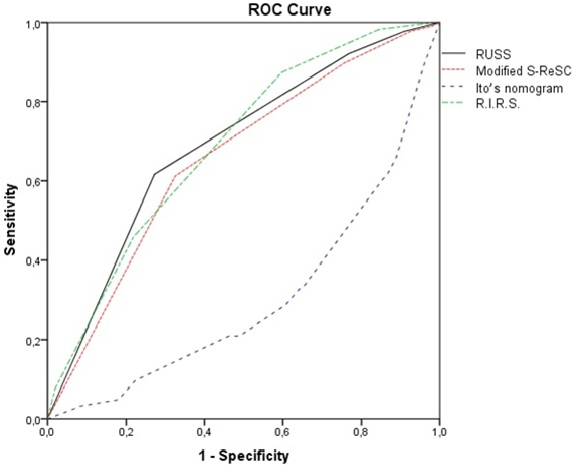
Objectives: To externally validate and compare Resorlu-Unsal stone score(RUSS), modified Seoul National University Renal Stone Complexity Score(S-ReSC), Ito’s nomogram and R.I.R.S. scoring systems for predicting capabilities of both the stone-free status and complications in a multi-institutional study. Materials and Methods: We performed a retrospective analysis of 949 patients who were underwent flexible ureterorenoscopy (f-URS) and laser lithotripsy for renal stones in two institutions between March-2015 and June-2020. The RUSS, modified S-ReSC, Ito’s nomogram and R.I.R.S. scores were calculated for each patient by same surgeon on imaging methods. Results were compared for their predictive capability of stone-free status and complications. Results: Of 949 patients 603 were male and 346 were female with a mean age of 47.2±14.3 (range 2-84years). Mean stone burden was 102.6±42.2 (48-270mm2). All nomograms predicted stone-free status (AUC were 0.689, 0.657, 0.303 and 0.690, respectively). All four scoring systems predicted complications with AUC values of 0.689, 0.646, 0.286 and 0.664 for RUSS, modified S-ReSC, Ito’s nomogram, R.I.R.S., respectively. Although all scoring systems were able to predict complications only Ito’s nomogram was able to predict Clavien ≥2 complications. Conclusion: All four scoring systems (RUSS, modified S-ReSC, Ito’s nomogram and R.I.R.S.) could predict stone-free status after f-URS, however the AUC values are not satisfactory in our large patient cohort. Although these scoring systems were not developed for predicting post-operative complications, they were associated with complications in our study. However, these four scoring systems have some significant limitations. The ideal scoring system is yet to be developed.