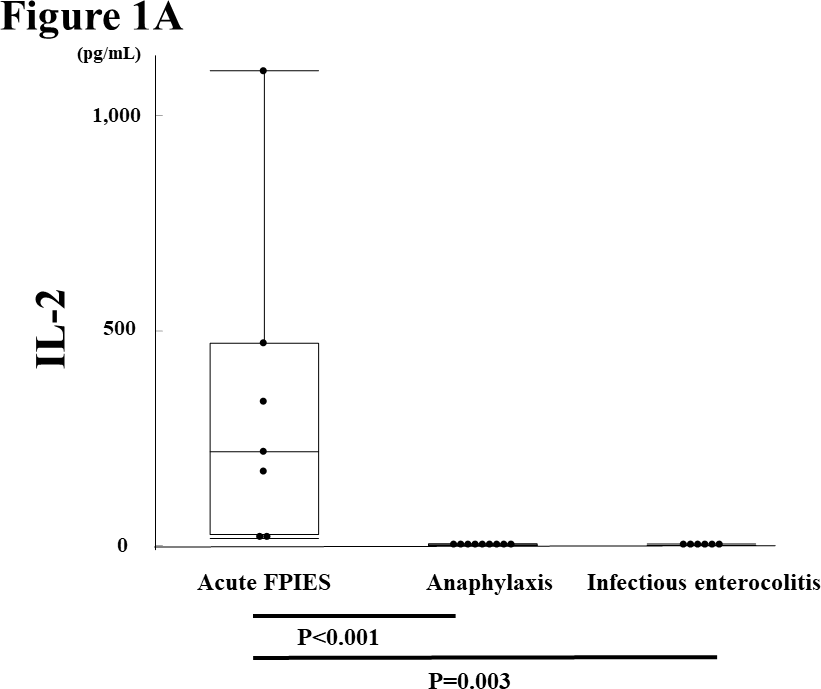
Background: Food protein-induced enterocolitis syndrome (FPIES) is a non-IgE cell-mediated food allergy characterized by repetitive vomiting and other gastrointestinal symptoms. Although little is known about FPIES pathophysiology, some cytokines have been reported to be involved. Since one of the main symptoms is vomiting, which is common to other diseases, it is difficult to distinguish acute FPIES from other conditions such as infectious enterocolitis. Thus, specific biomarkers are required for differential diagnosis. We aimed to identify potential biomarkers distinguishing acute FPIES from infectious enterocolitis and IgE-mediated anaphylaxis, which also cause vomiting. Methods: Seven patients with acute FPIES, nine with IgE-mediated anaphylaxis, and six with infectious enterocolitis were enrolled. The serum concentrations of interleukins (IL)-2, -4, -6, -8, -10, interferon-γ, and tumor necrosis factor-α were measured and compared among the three groups of patients. The serum concentrations of IL-2 and IL-10 were also compared between the symptomatic and asymptomatic stages. Alterations in serum cytokine levels were evaluated in acute FPIES during an oral food challenge test. Results: Serum IL-2 and IL-10 levels were significantly higher in acute FPIES patients than in patients with infectious enterocolitis and IgE-mediated anaphylaxis, whereas no significant differences were detectable in the serum levels of the other cytokines. The IL-2 and IL-10 elevation was only observed in the symptomatic stage of acute FPIES. Conclusion: The elevation in serum levels of IL-2 and IL-10 was specifically observed in symptomatic acute FPIES cases, suggesting that the measurement of IL-2 and IL-10 could be employed for differential diagnosis.