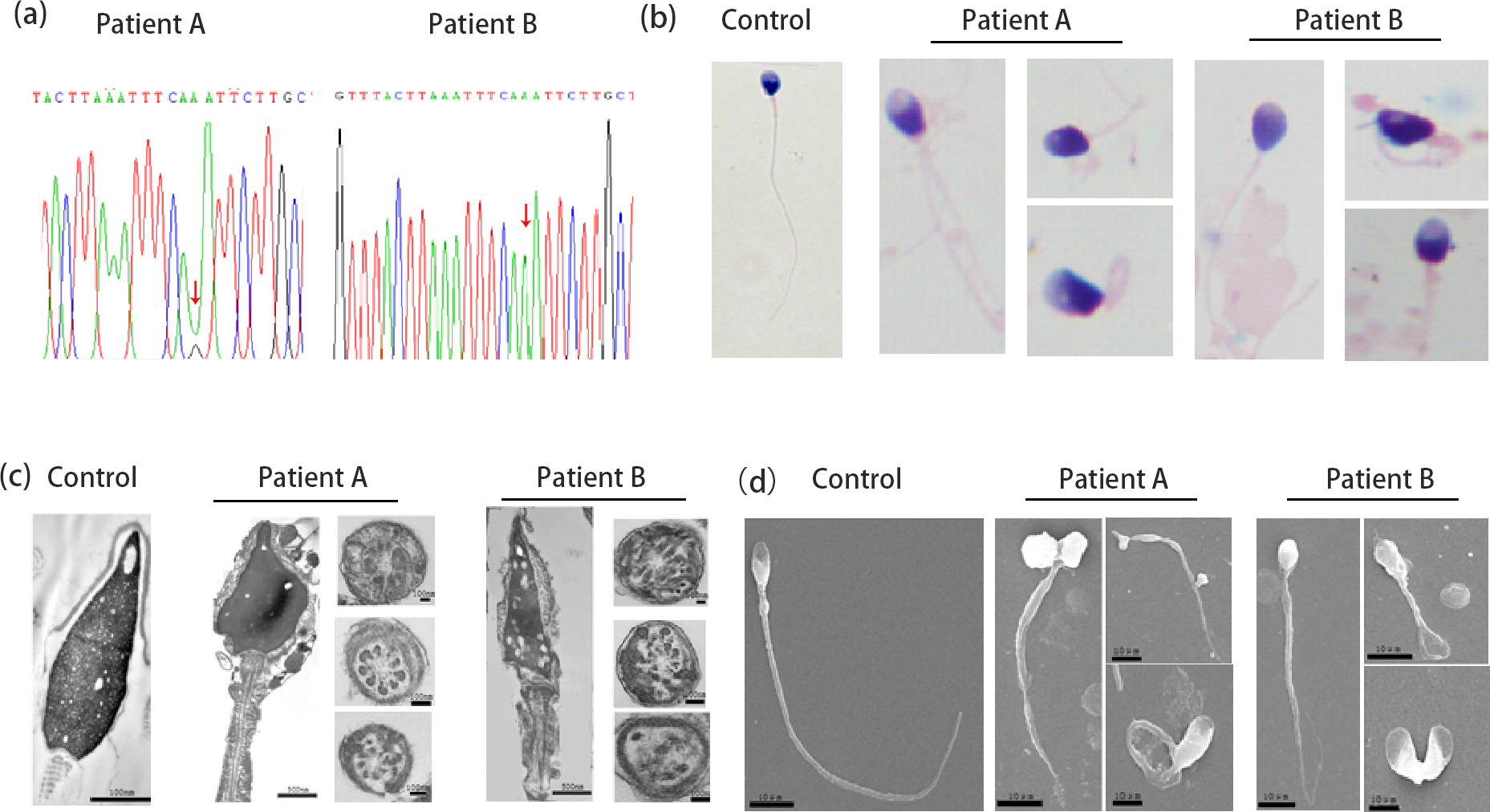
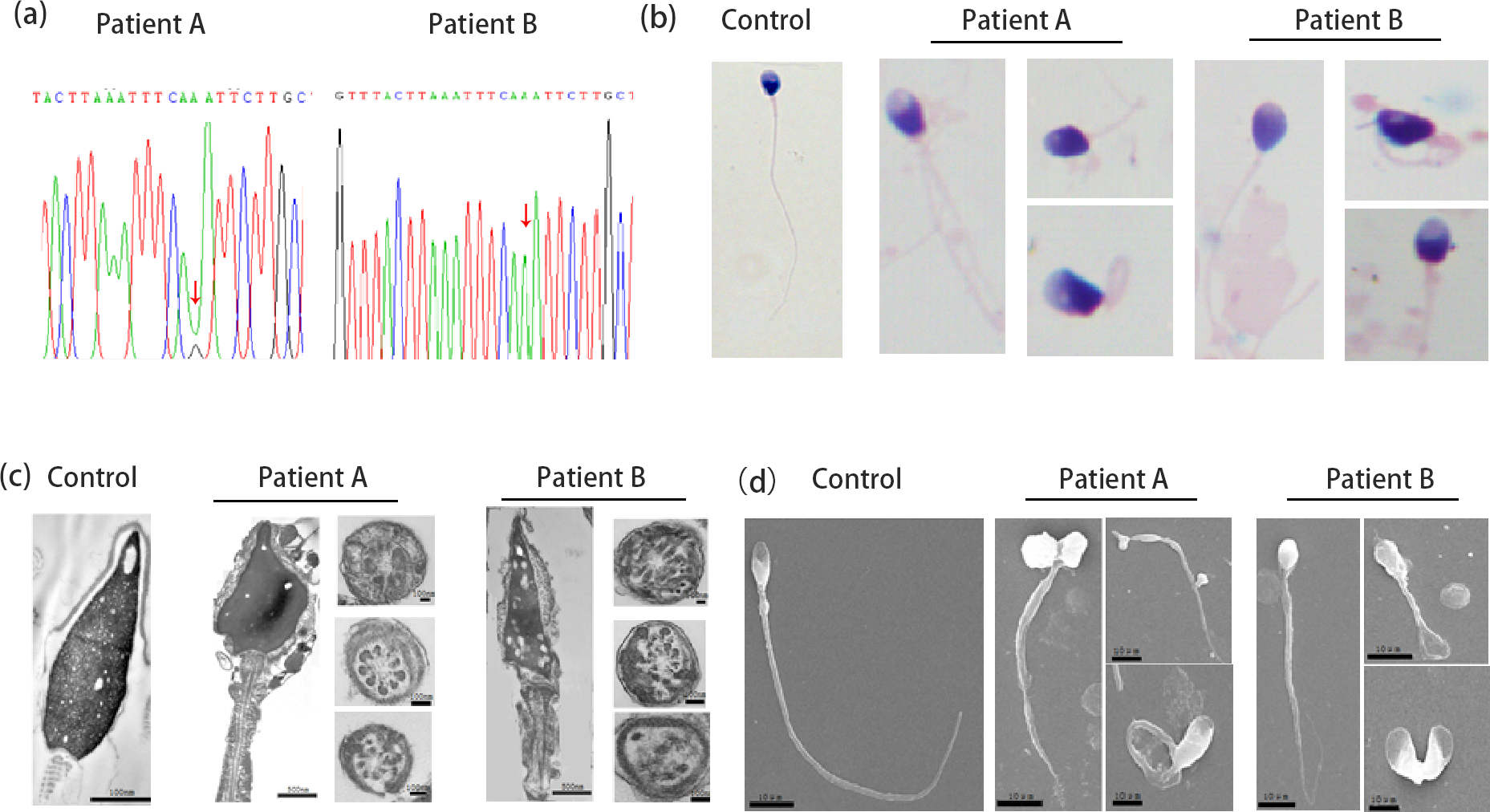
Concern the pathogenicity ofheterozygous mutation c.346-1G>A in SOHLH1 gene for NOAMohan Liua,b#, Ying Shenb#, SuRen Chenc*, Yihong Yangd*a State Key Laboratory of Biotherapy and Cancer Center, West China Hospital, SichuanUniversity and Collaborative Innovation Center, Chengdu 610041, China.b Department of Obstetrics/Gynecology, Joint Laboratory of Reproductive Medicine (SCU-CUHK), Key Laboratory of Obstetric, Gynecologic and Pediatric Diseases and Birth Defects of Ministry of Education, West China Second University Hospital, Sichuan University, Chengdu 610041, Chinac Education Key Laboratory of Cell Proliferation & Regulation Biology, College of Life Sciences, Beijing Normal University, Beijing 100875, Chinad Reproduction Medical Center of West China Second University Hospital, KeyLaboratory of Obstetric, Gynecologic and Pediatric Diseases and Birth Defects ofMinistry of Education, Sichuan University, Chengdu 610041, China# These authors contributed equally to this work*Correspondence should be addressed to: SuRen Chen: chensr@bnu.edu.cn; Yihong Yang: zxgo88@163.comTo the Editor:We have noticed that Choi Y et al. reported the heterozygous mutation in SOHLH1 gene (NG_033784.1: c.346-1G>A) caused the original splicing site disruption and partial deletion within exon 4, thus generated a truncated bHLH domain and resulted in nonobstructive azoospermia (NOA) in two Korean patients (Choi et al., 2010). The authors also performed hematoxylin-eosin staining (H&E) to exam patient’s testis and the result showed a severe dysfunction in spermatogenesis characterized by no spermatogonia, spermatocyte, spermatids, or mature spermatozoa. Therefore, the author assumed this heterozygous mutation inSOHLH1 resulted in NOA due to the absence of normal spermatogenesis.We would like to bring to your attention that we found this heterozygous mutation in a Chinese patient A by whole-exome sequencing (WES) (Figure 1a). This patient did not suffer from NOA, whose sperm concentration and sperm count were normal but had almost no motility (Table 1). Particularly, most of the sperm from patient had amorphous head and the anomies in flagella compared to the normal control by Papanicolaou staining (Figure 1b). Moreover, scanning electron microscopy (SEM) further confirmed that the sperm of patient had aberrant head including round-head, double-head, tapered-head, pyriform head and/or irregular head with short, bent, coiled and flagella (Figure 1c). Additionally, we analyzed the ultrastructure of the patient’s spermatozoa as well as the normal control by transmission electron microscopy (TEM). TEM analysis screened normal spermatozoa had proper ratio of head’s length to width, and the 9+2 structure (nine peripheral microtubule doublets and two central microtubules, surrounded by outer dense fiber and fibrous sheath) was integrated and regularly arranged. For patients, we observed that sperm plasma membrane was swollen and damaged, cell nucleus contained vacuoles, and mitochondria was empty foamed, combined with an atypical 9+0 arrangement of axonemal microtubules in the sperm flagella (Figure 1d). According to these findings, we speculated that patient A suffered from teratozoospermia but not NOA.Remarkably, we detected a homozygous mutation of c.346-1G>A in SOHLH1 gene in another Chinese patient B (Figure 1a). For this patient, his sperm count was extremely low. In addition, we found his sperm morphology was also abnormal. Though Papanicolaou staining, we observed deformities of head and flagella (Figure 1b). SEM and TEM further identified abnormality of sperm morphology and defective sperm ultrastructure (Figure 1c and d). Thus, patient B was affected to severe oligozoospermia. Although c.346-1G>A in SOHIL1 gene is a deleterious mutation which disrupted splice site, we have provided evidence that heterozygous c.346-1G>A in SOHIL1 gene was not responsible for NOA, and homozygous mutation led to severe oligozoospermia.SOHLH1 is a transcription factor which specifically expresses in germ cells, and plays an important role in the development of spermatogenic cells through transcriptional regulation of downstream genes such as SYCP1 (Ballow D et al., 2006; Li et al., 2019). Some researchers have focused on the relationship between SOHLH1and male infertility. Sohlh1 knockout male mice (Sohlh1-/- ) had a large number of apoptotic spermatocytes in the meiotic stage, resulting in failure of spermatogenesis and led to male infertility (Li et al., 2019). Similarly, our patient B carrying homozygousSOHLH1 mutation showed the severe reduction in total sperm number. Considering the low homology of SOHLH1 gene in humans and mice (https://www.ncbi.nlm.nih.gov/homologene/), it is reasonable that there are some differences in phenotypes between humans and mice with homozygous variation of SOHLH1 , but both due to a decrease in the number of spermatozoa. However, Li et al. didn’t mention any sperm parameter about heterozygous male mice, and we speculate that heterozygous male mice had normal fertility thus could produce the homozygous mice. Moreover, our patient A with the heterozygous mutation showed the normal sperm number. All the observations might be explained that another normal allele of SOHLH1 could totally translated into the intact protein and further performed normal biology functions, while the homozygous mutation led to the complete absence of SOHLH1 expression. What’s more, Song B et al. performed single nucleotide polymorphism (SNP) linkage analysis of SOHLH1 , and discovered that there was no relationship between the rs558113 in SOHLH1gene and susceptibility to NOA in Chinese population, suggesting that heterozygous mutation in SOHLH1 may not associated to NOA (Song et al., 2015). Moreover, no evidence suggests the SOHLH1 gene has haploinsufficiency (https://clinicalgenome.org/). Remarkably, patient A in our study followed ICSI, and his wife became pregnant and had successful delivery. This outcome strongly suggested patient A could select normal sperm to fertilization, and heterozygous mutation of c.346-1G>A in SOHIL1 gene didn’t result in NOA. Actually, we didn’t deny that heterozygous mutation of SOHLH1 has a certain degree of contribution to male infertility, and it may combine with other gene mutations or factors to drive the occurrence and development of NOA, or epigenetic modifications affect the gene transcriptional expression level.According to our evidences, the heterozygous mutation of c.346-1G>A in SOHIL1 was not the directly genetic cause for NOA. Due to the complexity of the spermatogenesis process, and the etiological factors of male infertility are mysterious, we should cautious about mutations which discovered in patients and performed more functional experiments to constitute the relationship between genotype and phenotype, so that we can provide more strong and accurate evidence for clinical diagnose.