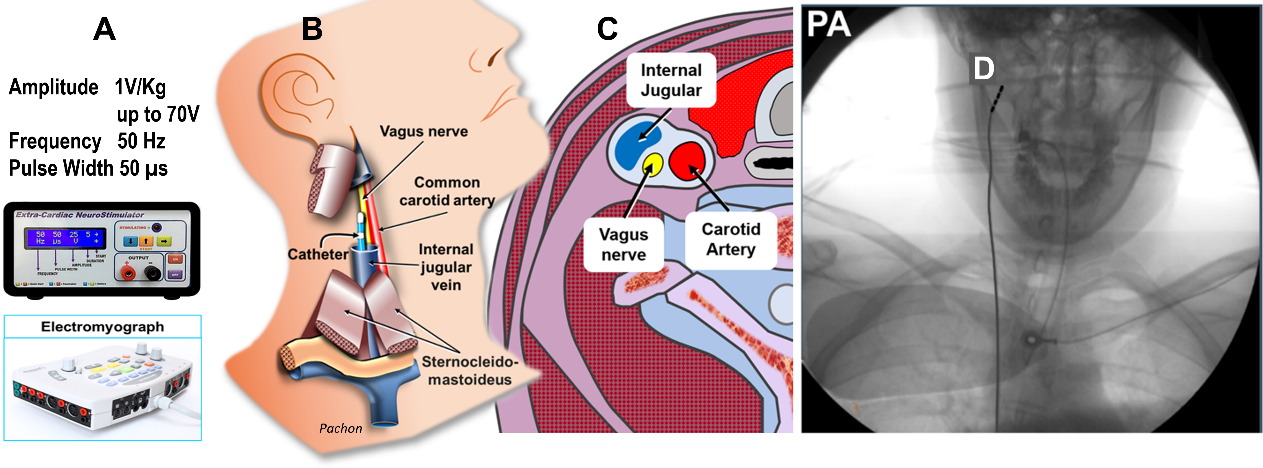
Background: The differential diagnosis of supraventricular tachycardias(SVTs) is essential during radiofrequency(RF) ablation. The Extracardiac Vagal Stimulation(ECVS), introduced in 2015, offers new insights for electrophysiologic studies and ablation by allowing a controlled vagal effect on the heart. Methods: A prospective study of 625 patients with SVT ablation indication. ECVS was performed using a regular electrophysiology catheter to study atrioventricular(AV) and ventriculo-atrial(VA) conduction and their effects on tachycardia. Baseline ECVS was performed to determine the optimal position for right or left ECVS, near the jugular foramen. ECVS was repeated during atrial and ventricular pacing(VP) to monitor the procedure’s progression and ensure successful endpoints. Results: ECVS was successful in 611/625 patients(98%), 381(62.3%) had AV node reentry tachycardia(AVNRT), and 230(37.6%) Accessory Pathway(AP), including 135(58.7%) manifest AP(WPW) and 95(41.3%) concealed AP. ECVS+VP in 33 patients with atypical AVNRT yielded VA block in 32(97%), suggesting VA conduction solely via the AV node. In contrast, 57 patients with concealed para-septal AP maintained VA conduction during ECVS, confirming AP. ECVS proved to be a fast, reliable, and practical additional EP tool: VA block indicated AVNRT, while persitent VA conduction suggested AP. Additionally, ECVS was highly effective in revealing and confirming successful AP ablation by demonstrating absence of AV and VA anomalous conduction. Conclusion: ECVS was a valuable tool in the diagnosis and ablation of SVTs. It allowed reproducible AV and VA block through normal pathways, easily identifying AVNRT and concealed, intermittent, or subtle AP. It was particularly useful in complex cases involving concealed AP and atypical AVNRT tachycardia.