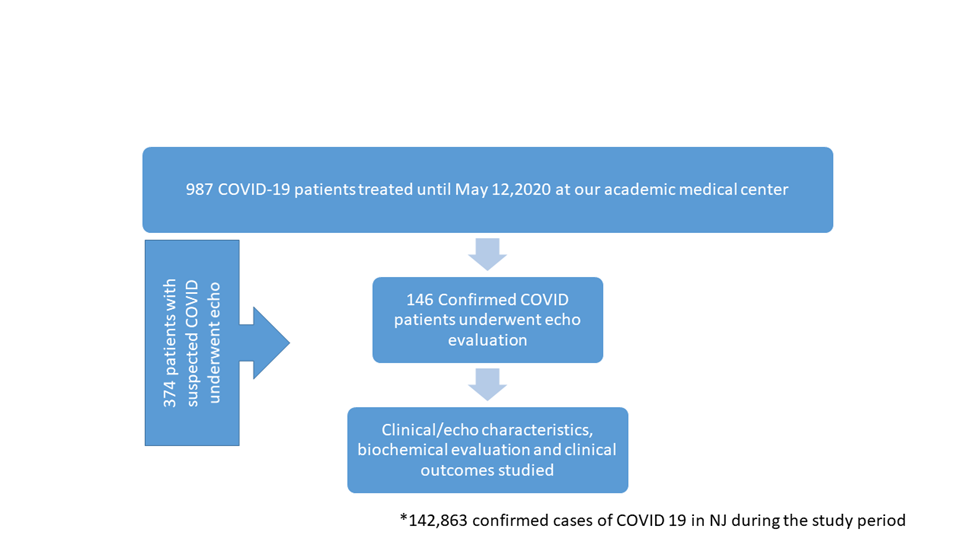
Background: Patients with cardiovascular disease are more susceptible to coronavirus disease 2019 (COVID-19) and have worse outcomes when infected. This study reports the largest and most comprehensive echocardiographic evaluation of patients with severe COVID-19 at a quaternary care hospital in the second most affected state in the US, New Jersey. Methods: Clinical, biochemical and echocardiographic features of consecutive patients with severe COVID-19 undergoing echocardiography were studied. Clinical outcome data including length of stay, requirement of mechanical ventilation and in-hospital mortality were collected. Results: 987 patients with confirmed COVID-19 infection were treated at our institution of which 146 consecutive patients (15%) underwent echocardiographic evaluation. Median age was 63 years ;37% were females, 21% had known CAD and 20% had CKD. 57% of patients required mechanical ventilation and 50% required vasopressors . 31% of patients died during the index hospitalization. There was a high prevalence of echocardiographic abnormalities including right ventricular dilation (33%) or dysfunction (21%), left ventricular dysfunction (20%), and pericardial effusion (13%). Multiple biomarkers including troponin T, pro BNP, dimer and CRP were strongly associated with echocardiographic abnormalities and in-hospital mortality. On Cox regression analysis, age (HR 1.04/year) and CAD (HR 2.4) were independent predictors of mortality. Conclusions: Severe COVID-19 infection is accompanied by a significant burden of echocardiographic abnormalities that are strongly correlated with higher degrees of inflammation and biomarker elevation. Additional investigation is warranted in assessing the role of a biomarker-guided approach for early cardiac surveillance using echocardiography in further risk stratifying patients and tailoring adjunctive therapy.