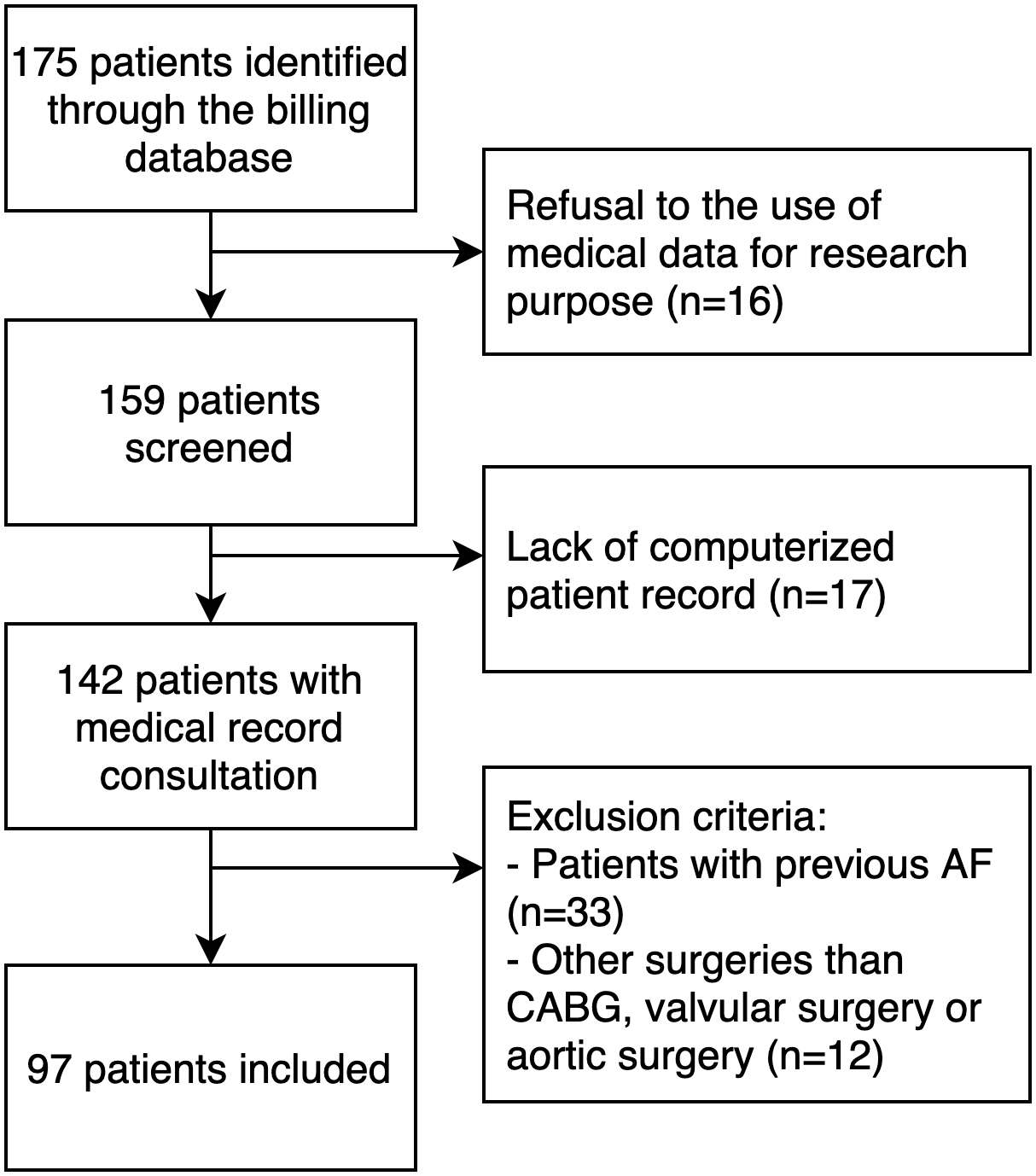
Rationale, aims and objectives: Postoperative atrial fibrillation (POAF) is the most common complication occurring after cardiac surgery. Guidelines for the management of this complication are scarce, often resulting in differences in treatment strategy use among patients. The aims of this study were to evaluate the management of POAF in a cardiac surgery department, characterise the extent of its variability and develop a standardised protocol. Methods: Data from patients who underwent cardiac surgeries with subsequent POAF between 1 January 2017 and 1 June 2018 were analysed in this single-centre observational retrospective study. The primary outcome was the difference in the proportions of patients whose first POAF episodes were treated with a rate control (RaC) strategy, a rhythm control (RhC) strategy and both among hospital units (intensive care unit [ICU], intermediate care unit [IMCU] and general ward [GW]). Secondary outcomes included the mean duration of POAF episodes, POAF recurrences, and the management of anticoagulation. Results: Data from 97 patients were included in this study. The POAF management strategy differed significantly among hospital units (ICU: RhC 75.0%, RhC and RaC 19.4%, RaC 0.0%; IMCU: RhC 40.4%, RhC and RaC 34.6%, RaC 13.5%; GW: RhC 22.2%, RhC and RaC 33.3%, RaC 44.4%; p = 0.001). Ninety-five (97.9%) patients converted to sinus rhythm after the first POAF episode; 51.2% of these conversions occurred within 8 h after onset. POAF recurred in 56.7% of patients. Considering all POAF episodes, 83 (85.6%) patients received amiodarone as part of the RhC strategy. Based on these results, a hospital working group developed a standardised protocol for POAF management. Conclusions: POAF management was heterogeneous at our institution. This paper highlights the need for clear practice guidelines based on large prospective studies to provide care according to best practices for all patients undergoing cardiac surgery.