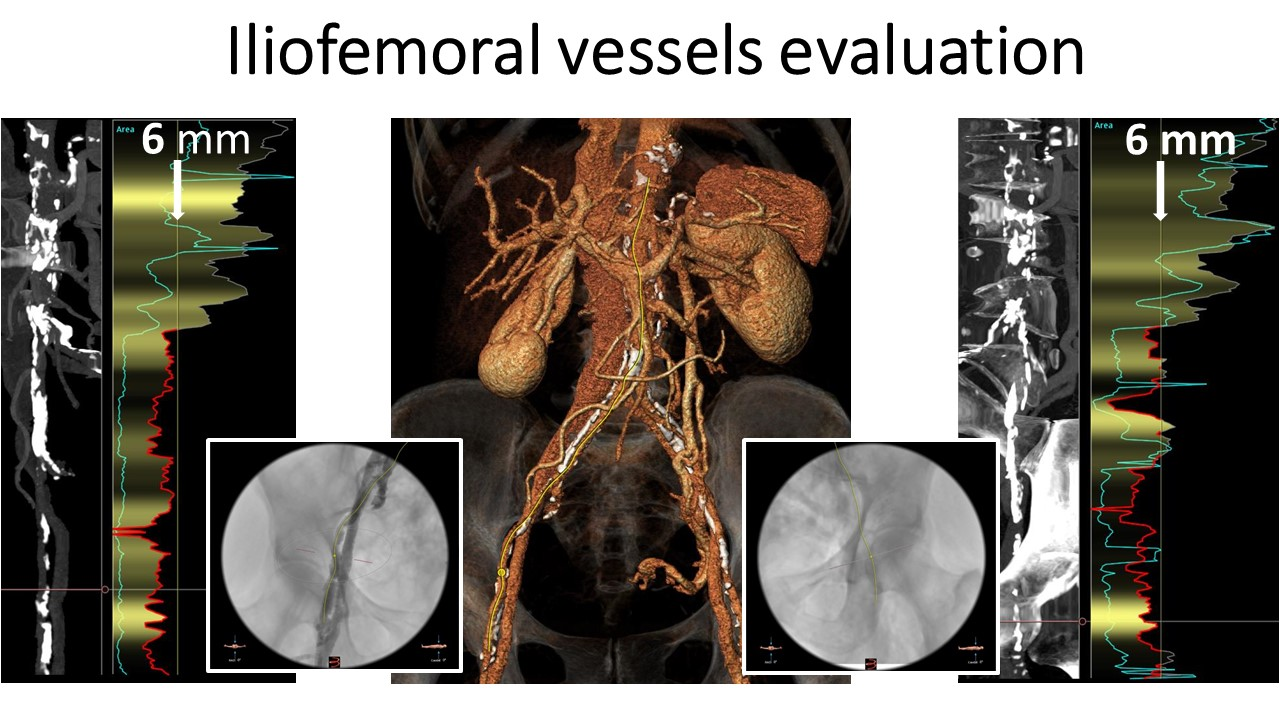
LETTER TO THE EDITOR RESPONSEWe thank Dr. Del Giglio et al. for their comments. As it was stated in our paper1, our primary goal was to describe our approach and procedural details to MIAVR by way of RALT. For further reading we would also like to draw attention to our video tutorial regarding RALT-MIAVR2. Nevertheless, we would like to congratulate Dr. Del Giglio and his colleagues for their significant contribution to the field of minimally invasive aortic valve treatment3 4 56.We completely agree with Dr. Del Giglio et al. that our statement regarding preoperative CT-scanning being mandatory is somehow misleading. However, other colleagues also consider a preoperative CT scan obligatory for RALT-MIAVR7 providing important additional information over TEE8. Three-dimensional reconstructed multidetector CT images allow virtual planning of the exposure leading to a reduced ischemia time and a reduced conversion rate9. It has also been shown that systematic preoperative CT screening in MIMVS is associated with lower risk of postoperative stroke and a trend towards lower operative mortality10. Although we agree with Dr. Del Giglio et al. that CT assessment is helpful at the beginning, it remains accommodating throughout the complete learning curve and thereafter. Andre Plass et al.11 wrote that preoperative planning with multi-slice CT leads to an improved mental preparation and to an efficient and accurate surgical strategy including the choice of the optimal ICS. In their Letter to the Editor , Dr. Del Giglio et al. wrote that surgical access site selection does not require a CT scan, that the third ICS is the right one in most cases and that the surgeon could easily change to the second ICS from the same skin incision. We agree that changing ICS is easily possible, yet it also means added surgical damage and this should be avoided whenever possible. An automated method determining the closest ICS to the STJ as the optimal incision location for MIAVR has already been introduced12. A novel MIAVR tool that combines 3D imaging with quantitative planning measures has also been described13. The access angle is strongly associated with procedure complexity13 and with CPB time, x-clamping time and access difficulty13. Moodley et al.14 reported that mandatory CT-screening of the chest, abdomen and pelvis revealed significant subclinical aorto-iliac atherosclerosis resulting in a change in surgical approach in 21% of asymptomatic or mildly symptomatic patients scheduled for MIMVS (Figures 1 through 3). Regarding the interpreting and reconstructing of CT scans we agree with Dr. Del Giglio et al. that this means technological skills, time and financial resources. But with transcatheter cardiac procedures becoming more popular, it is important for the society of surgeons to master all aspects of case planning, which not only includes analysis and measurement but also the reconstruction of CT scans. As pointed out by Dr. Del Giglio et al. MIAVR has to reproduce the gold-standard conventional procedure in terms of safety, effectiveness and especially operative times through a respectful approach; yet in our opinion, preoperative non-invasive CTA screening in every patient scheduled for a RALT-MIAVR procedure remains crucial.In view of truly MIAVR, we believe that arterial and venous central cannulation both at the same time through the same incision does not reduce surgical trauma and could lead to central working port obstruction or significant narrowing. We believe that peripheral cannulation of the femoral vasculature is as safe and reproducible as central cannulation if the individualized anatomical characteristics allow for it. When carrying out percutaneous femoral arterial cannulation, we never perform a blind puncture of the femoral vessels. We prefer to have zoomed-in snapshots from our reconstructed CT scans on display in the OR to accurately puncture the CFA as displayed in figures 1 and 2 for example. Data set published by Eugene A. Grossi et al.15, suggest that if in older patients a femoral perfusion technique is chosen, preoperative evaluation of the aorta and distal vasculature would demonstrate that a given patient would not be at increased neurological risk15. This would include CTA of the aorta with runoff and TEE evaluation of the descending aorta15. They also published that RAP is associated with an increased risk of stroke in patients with severe PVD and should be reserved for selected patients without significant atherosclerosis. Such a thoughtful screening approach has been used also by Murphy and associates16 in robotic mitral valve surgery for example15. M. Murzi et al.17 were able to show that the use of RAP in MIMVS was associated with a higher incidence of neurological complications in older patients (>70 years old) with atherosclerotic burden compared with AAP. Still, their study had several limitations as it was based on a retrospective analysis of patients undergoing consecutive MIMVS over a 12-year period and potential bias might have been present17. The observational retrospective analysis of K. Bedeir et al.18 proved that femoral artery cannulation may be associated with increased stroke rates in isolated mitral valve surgery and that antegrade arterial cannulation (direct aortic or axillary cannulation (figure 2)) may be preferable in MIAVR. However, their consensus was that these preliminary data should trigger a larger-scale randomized prospective trial to confirm or refute these findings18.In pursuance of reducing hemolysis during CPB19, body temperature is maintained at around 34°C and DO2-guidance (goal-directed-perfusion). This is also helpful in regard to optimal venous drainage as it allows the surgeon1,2, to safely reduce the calculated pump flow. Furthermore, we augment venous drainage with the use of vacuum assistance (−20 to −35 mmHg) to decompress the right heart1. On one hand, R.K. Mathews et al.20 were not able to show a significant increase in hemolysis or sub-lethal red blood cell membrane damage, associated with the use of augmented venous drainage. On the other hand, D. Goksedef et al.21 showed that based on their results, negative suction at 80 mmHg may cause greater hemolysis than non-vacuum-assisted drainage or vacuum-assisted drainage at 40 mmHg. For this reason, we try to keep the vacuum assistance between 0 and -35 mmHg. Besides, it has been proved that application of a controlled, negative low pressure to the venous return does not cause hemolysis worse than gravitational CPB22.At last, Dr. Del Giglio et al. reported concerns about our SLL-PEEP (maximum 20 cmH2O) technique to inflate the left lung which pushes the aorta towards the surgical access. It is true that increased airway pressure or the application of high tidal volumes may cause damage or disruption of alveolar epithelial cells, by generating transpulmonary pressures that exceed the elastic properties of the lung parenchyma above its resting volume23. It has been demonstrated that the duration of mechanical stress defined as the stress versus time product affects the development of pulmonary inflammatory response23. However, in a recent meta-analysis of postoperative pulmonary complications after intraoperative ventilation, only a high driving pressure was associated with an increased incidence24. Therefore, it is highly unlikely that in an apneic patient on CPB, the elevation of the PEEP-level of 5 to 20 cmH2O without a resulting change of driving pressure has any significant negative effect on pulmonary outcome.In summary, we agree with the important points addressed by Del Giglio et al. Central cannulation and its AAP is possible without the need for preoperative CT scanning. However, for the sake of MIAVR (no rib resection, no IMA sacrifice) we prefer peripheral percutaneous cannulation. For such a RAP cannulation strategy, there is sufficient convincing literature that preoperative CTA scanning should be considered.