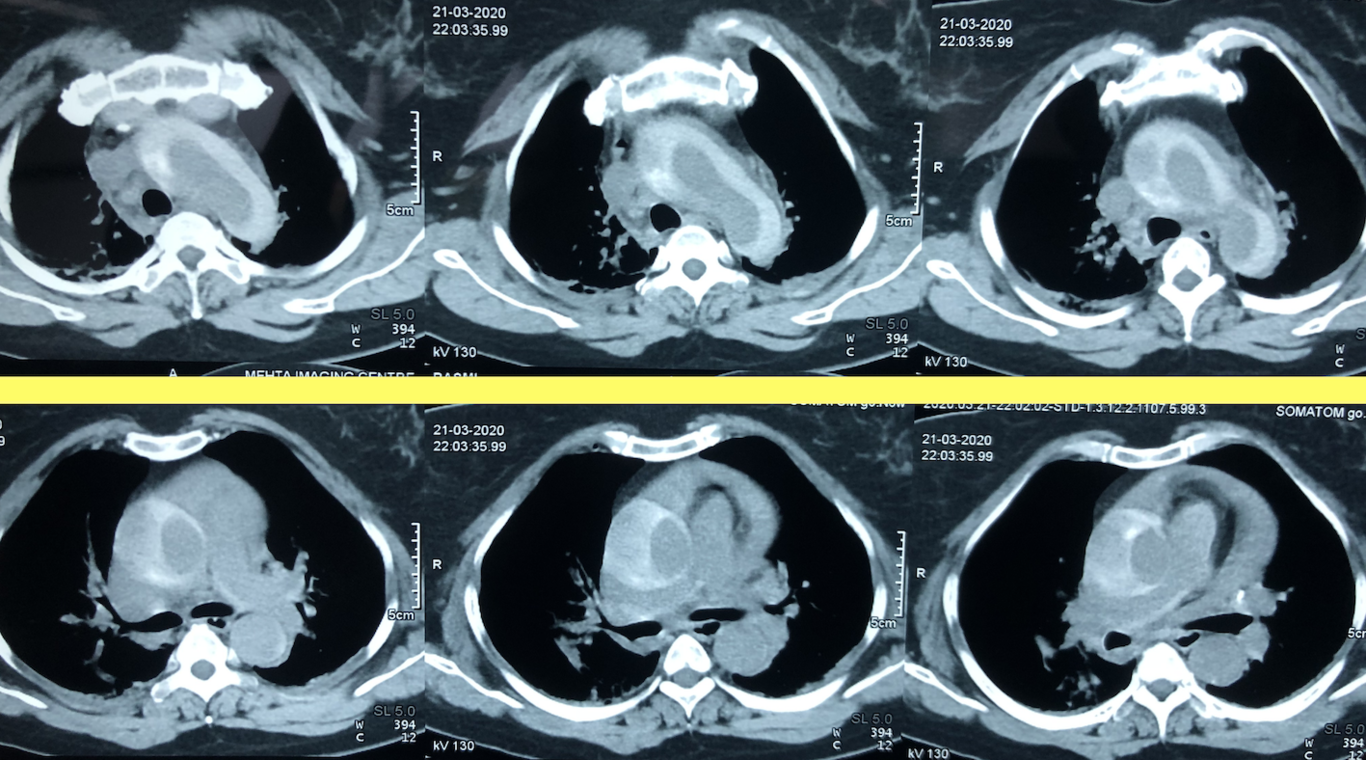
DISCUSSION – Left brachiocephalic vein is 6 cm long; it begins behind the sternal end of the clavicle, anterior to the cervical pleura by union of the left internal jugular vein and the left subclavian vein. It descends obliquely to the right, behind the upper half of the manubrium sterni, up to the sternal end of the first right costal cartilage, uniting here with right brachiocephalic vein to form SVC. The aortic arch is inferior to this vein. The left retro-aortic bracheocephalic vein is rare entity which was first described by Kerschner.[(1)](#ref-0001) Incidence of left retro-aortic bracheocephalic vein is noted between 0.2 to 1%.[(2)](#ref-0002) Aorto-pulmonary window is a rare cardiac condition, first described by Eliotson in 1830[(3)](#ref-0003) with an incidence of 0.2% - 0.3% of all congenital cardiac lesions.[(4,5)](#ref-0004) Three standard approaches for surgical closure of aorto-pulmonary window have been described in literature include: trans-aortic approach, trans-window approach, trans-pulmonary approach. Trans-window approach is also known as sandwich repair of aorto-pulmonary window.[(6)](#ref-0006) The left retro-aortic brachiocephalic vein with tetralogy of fallot and coarctation of aorta are noted. The left retro-aortic brachiocephalic vein with aorto-pulmonary window is very rare case and has not been reported previously. In our case the patient was admitted for AP window closure after complete pre-operative evaluation. Cardiac computed tomography reported 2.2cm aorto-pulmonary window with the left retro-aortic brachiocephalic vein. After obtaining parental consent for surgery, median sternotomy was performed. Thymus was excised and pericardium was opened longitudinally. By careful dissection, the left brachiocephalic vein was identified behind the distal ascending aorta adjacent to the AP window. Aorta was dissected off the brachiocephalic vein meticulously. Due to left retro-aortic brachiocephalic vein, aortic cannulation had to be done more caudally to avoid obstruction of vein. Aorta was cannulated and clamped without injury to the brachiocephalic vein. Attention was paid to avoid injury of the brachiocephalic vein during encircling the SVC for snaring. Aorto-pulmonary window was closed with PTFE patch through trans-window approach under mild hypothermia.[(6)](#ref-0006) Clinical implication of retro-aortic brachiocephalic vein is very important. More caudal cannulation of SVC is required in left brachiocephalic vein; but in AP window setting, this is more difficult as work space for closure of the defect is also required. Injury may occur to the vein during clamping of aorta. Left retro-aortic brachiocephalic vein may cause technical difficulty during central venous line placement through left arm approach. CONCLUSION- Being the rarest combination of left retro-aortic brachiocephalic vein and aorto-pulmonary window, certain things have to be taken care of like clamping of aorta, SVC cannulation, central vein catheter insertion, snaring of SVC. Pre-operative CT scan is also important to avoid intra-operative surprises.