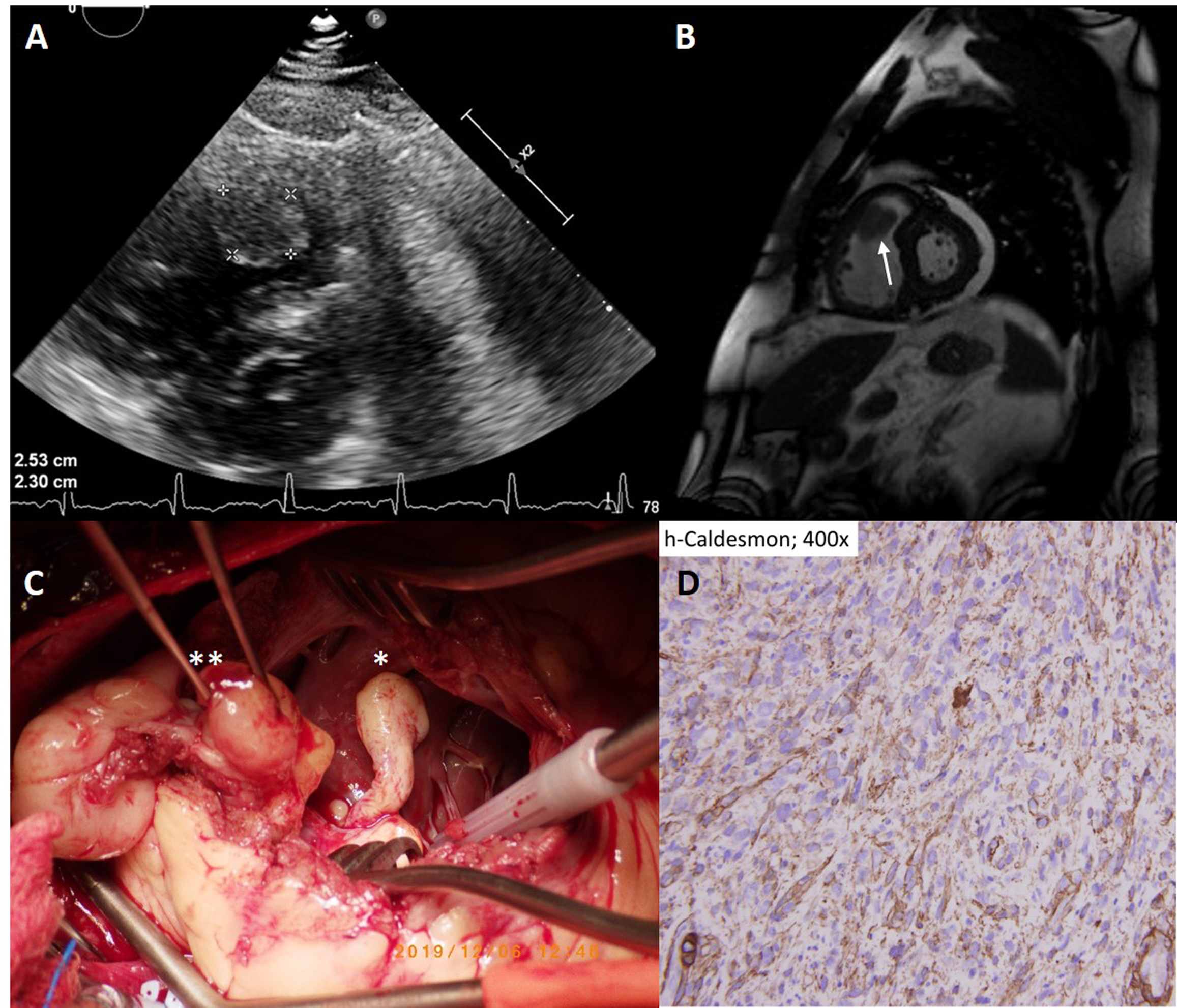
Primary cardiac leiomyosarcoma is not common but is lethal. Prompt surgery is mandatory for identifying the etiology while a comprehensive examination of pathology is crucial especially in the condition of two tumors with different etiologies. A 52-year-old man with medical history of systemic hypertension presented with chest discomfort and dyspnea. Echocardiography revealed the dilated right ventricle with a mass at right ventricular outlet tract (RVOT) (Figure 1A). It caused critical obstruction and resulted in severely pulmonary hypertension (estimated pulmonary systolic pressure up to 108mmHg). Cardiac magnetic resonance imaging confirmed a heterogeneous mass at RVOT with a high-intensity in T2 weighted image but failed to differentiate whether it is myxoma, metastasis or primary cardiac malignancy (Figure 1B). Given the exacerbating dyspnea, he received a prompt surgery which identified two tumors. One in the size of 9*4 cm originated from the RV dome extending to RVOT and pulmonary artery. The other smaller one (5*3 cm) mainly located within the RV (Figure 1C). The surgeon excised the smaller one for the frozen section while the immediate pathology reported that it was a benign lesion. Both tumors were removed. Surprisingly, post the operation the final pathology revealed that despite one tumor of benign degenerative tissues, the other of rare cardiac leiomyosarcoma at T1 stage. Immunohistochemical staining showed positive for smooth muscle actin and h-Caldesmon which is specific for leiomyosarcoma (Figure 1D). The patient subsequently received chemotherapies of Doxorubicin 75mg/m2 for 4 cycles.