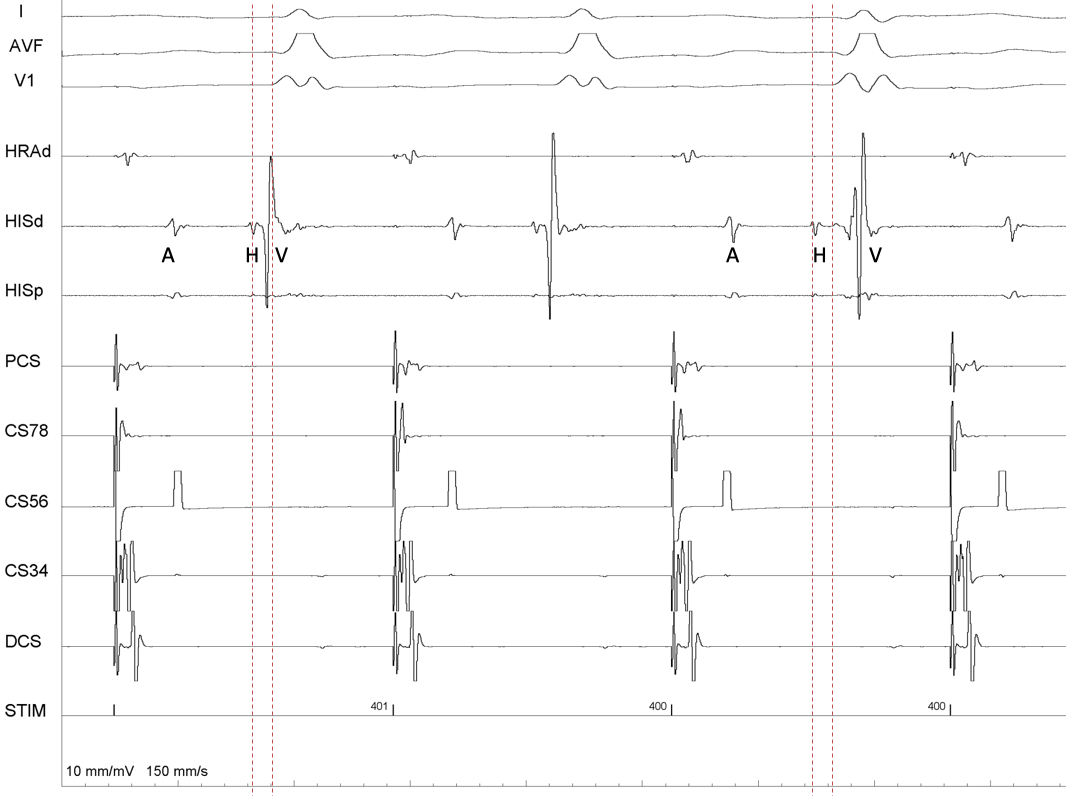
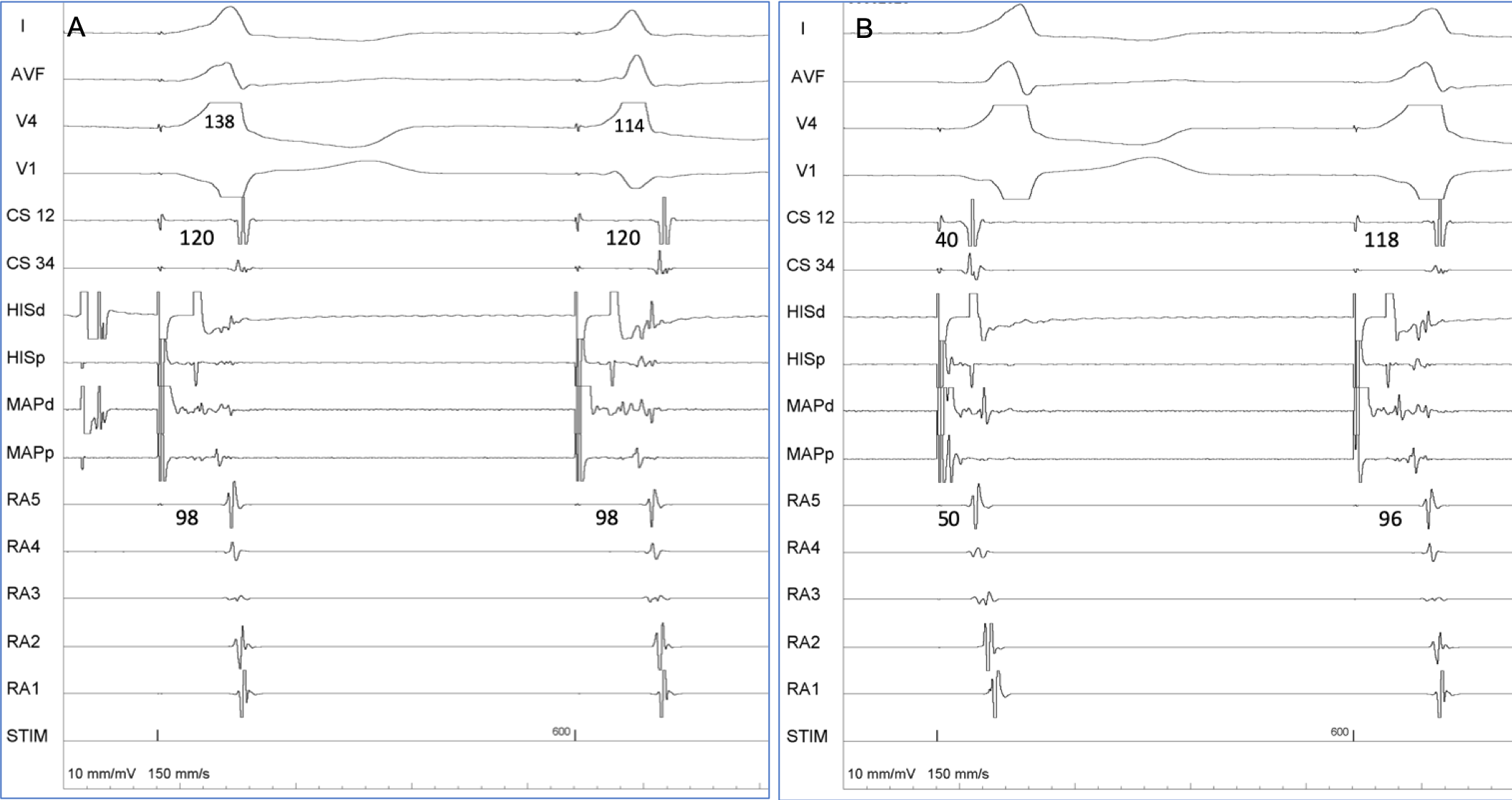
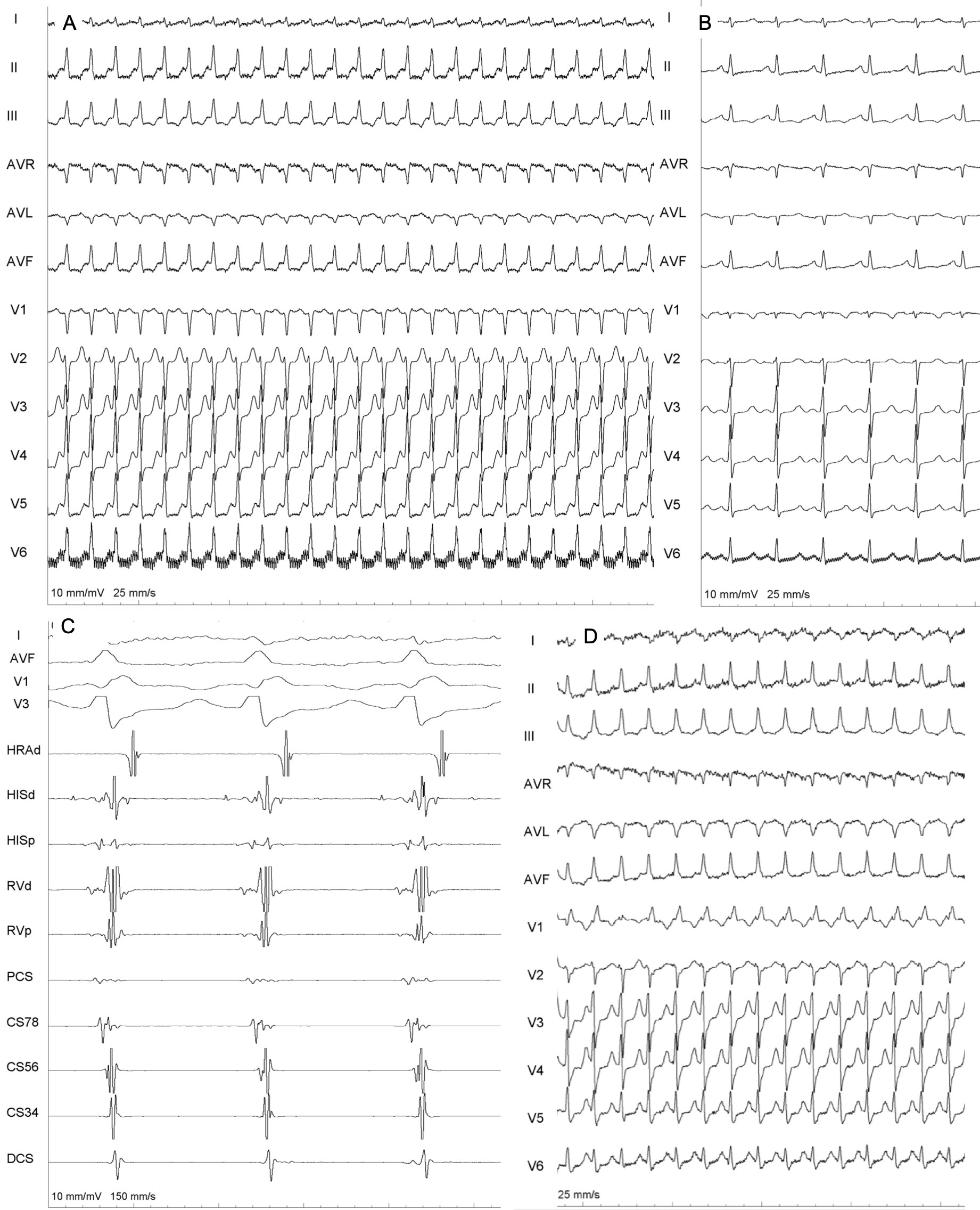
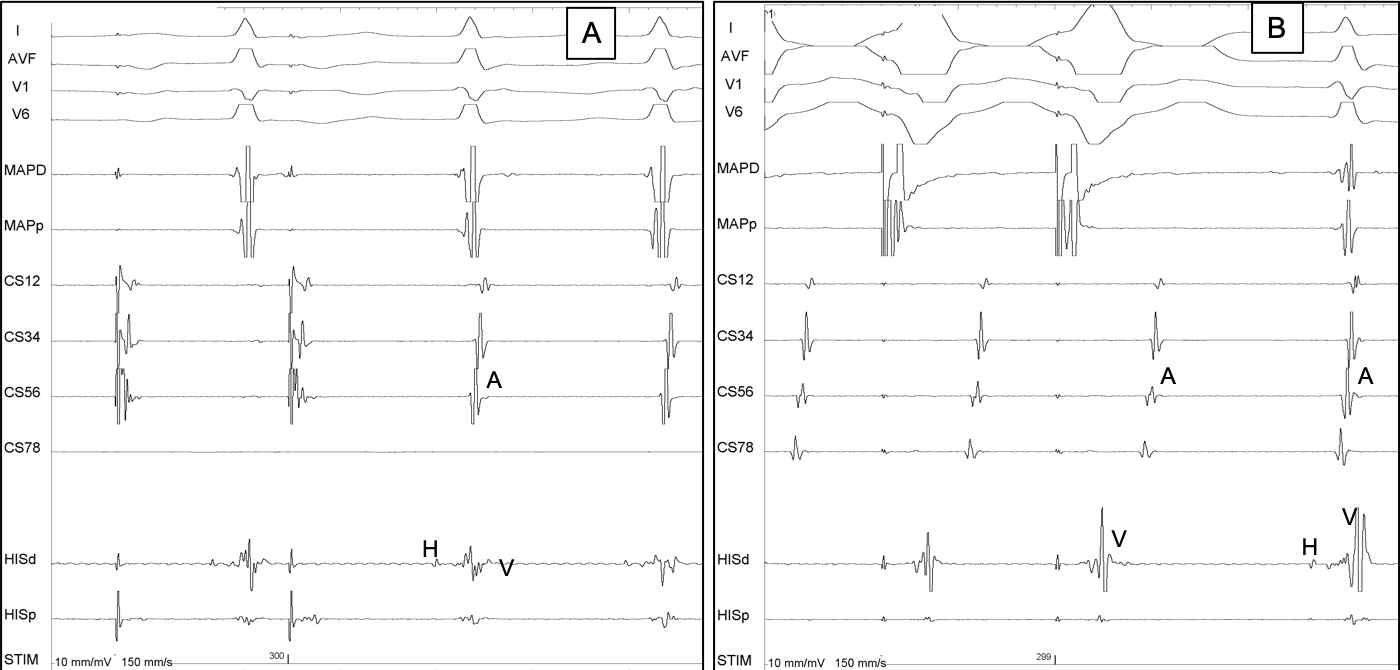
Case A 40-year-old gentleman underwent electrophysiology study for WPW syndrome with recurrent orthodromic atrioventricular reentrant tachycardia (AVRT). He had a right anterior accessory pathway (AP) which was ablated closer to the septum anterior to His catheter, ablation-distal (ABL) not recording any His signal during and after ablation (Appendix 1ABC). During the study, parahisian pacing (PHP) was performed before and after ablation as a routine protocol to determine the route of VA conduction (VAC). During the study 4 catheters were used: one quadripolar catheter for His region, One roving ablation catheter [for RV pacing/ mapping (MAP)/ablation], 2 decapolar catheters for coronary sinus (CS) and right atrium (RA). During PHP, both the His and MAP/ABL catheters were placed at His region. The CS catheter could not be placed fully deep inside, hence CS-12 was located near middle CS whereas the CS-34 was 2-3 cm inside proximal CS (Appendix 1BC). The decapolar catheter, placed in RA, was on the atrial aspect of tricuspid annulus, with RA-5 bipole near high right atrium (HRA). Pacing was performed at 600 ms cycle length (PCL) as her sinus CL was 700-750 ms. Starting at 20 mA current @ 2 ms pulse width and keeping the PCL and catheter position fixed, the current output was gradually reduced in a stepwise manner when various responses were noted. What are the responses observed in Fig.1 and Fig. 2?