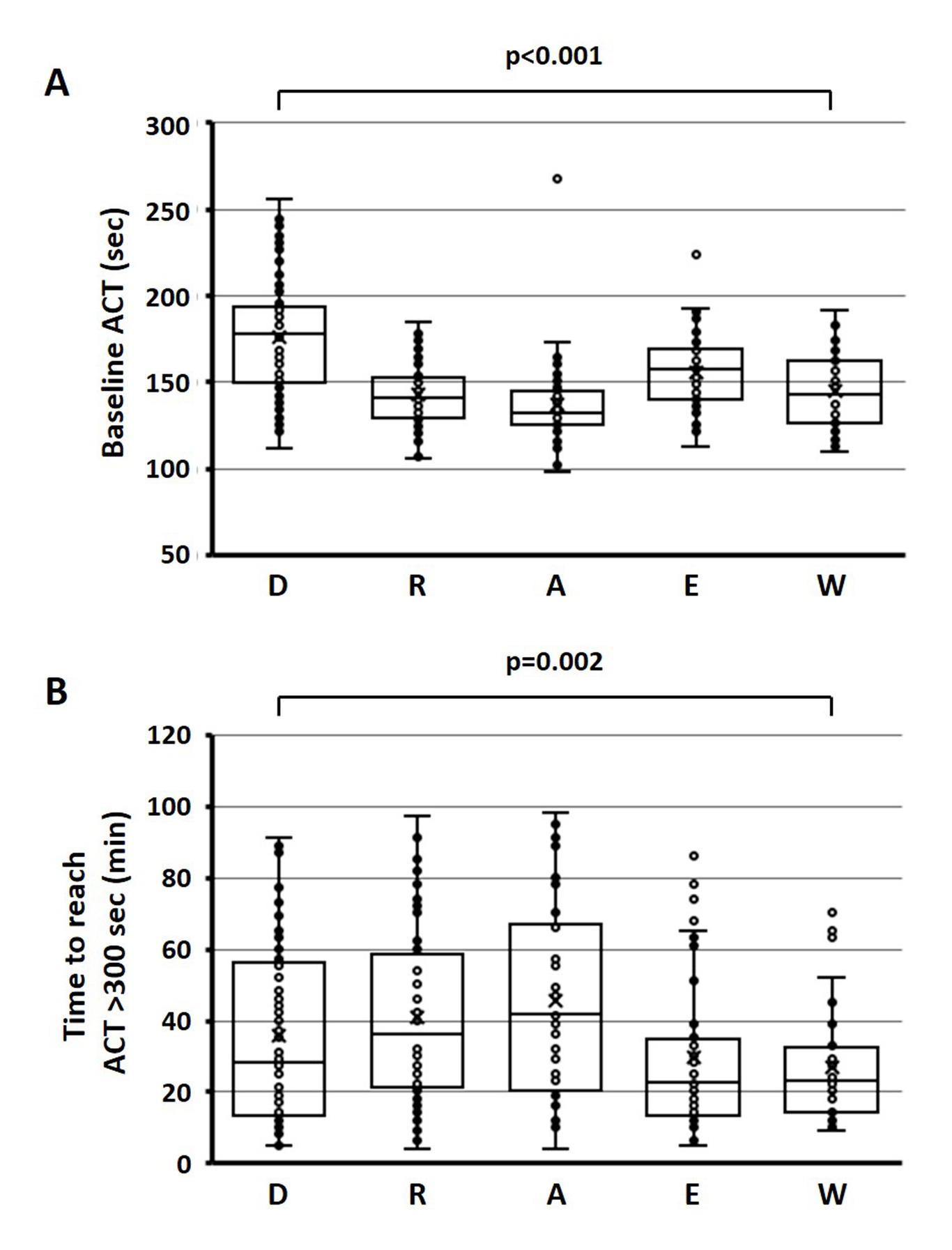
Introduction: Silent cerebral events (SCEs) are related to the potential thromboembolic risk in atrial fibrillation (AF) ablation. Peri-procedural uninterrupted oral anticoagulation (OAC) reportedly reduced the risk of SCEs, but the incidence still remains. Methods and Results: AF patients undergoing catheter ablation were eligible. All patients took non-vitamin K antagonist oral anticoagulants (NOACs, n=248) or vitamin K antagonist (VKA, n=37) for peri-procedural OAC (>4 weeks) without interruption during the procedure. Brain magnetic resonance imaging was performed within 2 days after the procedure to detect SCEs. Clinical characteristics and procedure-related parameters were compared between patients with and without SCEs. SCEs were detected in 66 patients (23.1%, SCE[+]) but were not detected in 219 patients (SCE[-]). Average age was higher in SCE[+] than in SCE[-] (66±10 years vs. 62±12 years, p<0.05). Persistent AF prevalence, CHADS2/CHA2DS2-VASc scores, serum NT-ProBNP levels, left-atrial dimension (LAD), and spontaneous echo contrast prevalence in transesophageal echocardiography significantly increased in SCE[+] vs. SCE[-]. SCE[+] had lower baseline activated clotting time (ACT) before heparin injection and longer time to reach optimal ACT (>300 sec) than SCE [-] (146±27 sec vs. 156±29 sec and 44±30 sec vs. 35±25 sec, p<0.05, respectively). In multivariate analysis, LAD, baseline ACT, and time to reach the optimal ACT were predictors for SCEs. The average values of the ACT parameters were significantly different among NOACs/VKA. Conclusion: LAD and intra-procedural ACT kinetics significantly affect SCEs during AF ablation. Different anticoagulants have different impacts on ACT during the procedure, which should be considered when estimating the risk of SCEs.